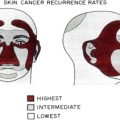
Atypical fibroxanthoma, malignant fibrous histiocytoma, sebaceous carcinoma, and extramammary Paget disease are rare cutaneous tumors. Their recognition and diagnosis are critical in decreasing long-term morbidity and mortality. Surgical excision is the treatment of choice for these tumors, and Mohs micrographic surgery has been shown to be as favorable or better than wide local excision in providing long-term clearance rates.
Atypical fibroxanthoma
History
Cutaneous sarcomas are primary skin neoplasms of nonepithelial cell origin. They are locally aggressive and have a varying capacity to metastasize. Atypical fibroxanthoma (AFX) is a cutaneous sarcoma of mesenchymal origin that has been referred to in the past by various names including pseudosarcoma and superficial malignant fibrous histiocytoma. It was first identified as a disease sui generis in the early 1960s by Helwig, who later described one of the largest series to date. It was once believed to be a benign local reactive proliferation until it was later evident that these tumors possess the capability to metastasize. Treatment of these sarcomas has included cryotherapy, radiation, wide local excision (WLE), and Mohs micrographic surgery (MMS).
Epidemiology
AFX arises most commonly in elderly white men with an overall male/female ratio approaching 7:1. The true male/female ratio may extend beyond this as most reports in the literature are on men. The prevalence seems to be bimodal with the highest frequency of tumors occurring in the seventh decade. These occur primarily on the ears, nose, and cheeks. A second smaller subset of patients, whose median age is within the fourth decade, develop AFX more commonly on the trunk and extremities. The true per capita incidence of AFX has not been meticulously defined given it is relatively uncommon and there is no registry available for these tumors.
Cause and Pathogenesis
AFX may represent a reparative or benign reactive process in previously damaged skin. Ultraviolet (UV) and ionizing radiation are both suspected factors for the development of AFX. Evidence supporting this includes their common occurrence on actinically damaged skin, as portrayed histologically by its background of elastosis. These patients also usually have a history of other malignancies instigated by UV radiation such as basal or squamous cell carcinoma. UV induction has been substantiated by the fact that some AFX have shown P53 gene mutations, specifically on dipyrimidine sites, and the production of cyclobutane pyrimidine dimers. Furthermore, AFX has been reported in patients with xeroderma pigmentosum who have an inability to repair UV-induced pyrimidine dimers.
Although generally not a biologically aggressive tumor, when not adequately treated AFX recurs locally in up to 20% of cases; local recurrence portends a significantly higher risk for metastasis. Time to recurrence may be extremely variable from within 2 months to 13 years, with the average time to recurrence being approximately 27.5 months. Although the exact rate of metastases is unknown, it is estimated to occur in 1% of cases. If metastasis does occur, it is within approximately 20 months of the original diagnosis. Factors that lend to higher metastatic potential and a poor prognosis include tumor extension into deep subcutaneous tissue, size, history of ionizing radiation, lymphovascular involvement, and immunocompromised state. Although local and distant metastases rarely occur, it seems that if metastases do occur they are to regional nodal beds.
Tumor depth plays an important roll in the diagnosis of AFX; at times with deeper tumors into fascial planes it is difficult to make a distinction between AFX and superficial malignant fibrous histiocytoma (MFH). This is an important differentiation because the diagnosis of MFH is much more ominous carrying a higher risk of metastasis and poorer prognosis. Because tumor depth in AFX is correlated with metastases, and because of the difficult distinction from superficial MFH, it is prudent to perform sentinel lymph node biopsy on patients with tumors that extend to deep subcutaneous levels. Sentinel lymph node biopsy may also be recommended for recurrent tumors, however locating the true sentinel node of the original tumor may be an arduous task because of disruption of the drainage patterns as a result of the primary procedure.
Clinical Features
The characteristic presentation of an AFX is that of a single firm painless friable nodule typically less than 2 cm in diameter ( Fig. 1 ). Ulceration may be present and bleeding may occur with minimal trauma. The most common locations are head and neck, but in younger patients they may be more common on the trunk and extremities.

Differential diagnosis includes, but is not restricted to, spindle cell squamous cell carcinoma, basal cell carcinoma, leiomyosarcoma, dermatofibrosarcoma protuberans, spindle cell or amelanotic melanoma, as well as the superficial portion of an underlying MFH.
Dermatoscopy may be a useful clinical tool when evaluating these tumors. Superficial white areas or a white veil may be seen. Areas containing polymorphous vascular structures, including dotted, globular, linear, tortuous, and arborizing patterns, can also be appreciated. Although not substantially specific, dermatoscopy may be added to the diagnostic armamentarium for these rare tumors.
Diagnosis
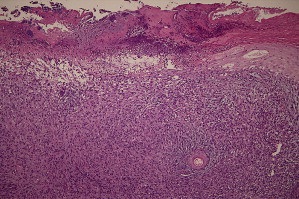
Histologic examination of AFX reveals a proliferation of pleomorphic atypical spindle and polygonal cells in a haphazard arrangement within a fibrous stroma; both of these cell types contain a high nuclear/cytoplasmic ratio, striking nucleoli, and coarse chromatin patterns. A high proportion of atypical mitotic activity is present ( Fig. 2 ). Abundant multinucleated giant cells are typical. Although rare, perineural invasion may be present. These features may be indistinguishable from those seen in MFH, which is why many consider AFX to be a variant of this deeper tumor.
Although not typically articulated, AFX has been subcategorized as being histiocyte predominant, spindle cell predominant with a smooth muscle-like pattern, spindle cell predominant with a storiform-like pattern, spindle cell predominant with course nuclear membranes resembling squamous cell carcinoma, and xanthogranulomatous. Other cellular variants have been described and include myxoid, pigmented, clear cell, those containing osteoclast-like giant cells, and granular cell types. Monomorphic spindle cells in a fascicular array with eosinophilic cytoplasm and high mitotic rate are seen in the spindle cell nonpleomorphic type; there is a lack of pleomorphism and this variant of AFX is frequently misdiagnosed.
Immunohistochemistry may be helpful in diagnosing AFX; vimentin, CD68, smooth muscle actin, α1-antitrypsin, α1-chemotrypsin, and factor XIIIa are often positive. Other stains that may highlight AFX include CD74, CD117, CD10, CD99, CD163, LN-2, and procollagen-1. CD10 may also be a useful immunohistochemical stain for Mohs sections. In the setting of a difficult to classify tumor, vigilance should be used when interpreting these stains because they do not possess a high degree of specificity. Cytokeratin, S-100 and HMB-45, desmin and calponin, and CD34 are characteristically negative and are helpful in differentiating spindle cell squamous cell carcinoma, desmoplastic melanoma, leiomyosarcoma, and dermatofibrosarcoma protuberans, respectively.
Treatment
As previously stated, AFX has been treated with cryotherapy, radiation, WLE, and MMS. Although reported to be efficacious in a small series, because of the risk of recurrence and metastatic potential with AFX, cryotherapy is discouraged. Irradiation is also not recommended because of the potential to further increase the aggressive behavior of the tumor.
WLE has long been the standard modality to treat AFX. Although recurrence rates ranging between 0% and 20% have been reported using WLE, there are sparse data describing the exact surgical margins taken for these tumors. True recurrence rate with WLE is likely around 10%. Excisions should extend to the fascial plane because of the potential depth of invasion and associated malignant potential if present. Although no definite surgical margins have been established, margins of at least 1 to 2 cm are recommended to acquire the highest potential clearance.
MMS offers the advantage of complete marginal examination as well as sparing of normal surrounding tissue. One hundred percent marginal assessment is extremely valuable because of the risk of metastasis with local recurrence. In addition, the subclinical spread of AFX may typically be greater than 1 cm, which is the margin that is usually taken during WLE. The mean number of Mohs levels needed to clear AFX is approximately 2. MMS has been shown to provide superior clearance rates over WLE for AFX. Because of the rarity of this tumor, the number and recurrence rate of AFX treated with MMS has varied in the few studies in which it has been evaluated; studies containing 5-year follow-up rates are also sparse. On average, the available follow-up for AFX treated with MMS is approximately 30.7 months; the average recurrence rate is 3%. Because local recurrence is so highly correlated with metastasis and overall survival, and because fewer recurrences are seen with MMS compared with WLE, MMS should be used to treat AFX when possible.
MFH
History
MFH was first described in 1961 by Kauffman and Stout; previously, it had been referred to by such names as fibroxanthoma, malignant fibrous xanthoma, malignant giant tumor of soft parts, and pleomorphic fibrosarcoma. MFH is best regarded as a soft tissue sarcoma and is now referred to by many as pleomorphic sarcoma. The questions surrounding its origin and its many subtypes have made the diagnosis of MFH as its own entity controversial. Although MFHs arise in subcutaneous tissue, they arise more commonly in soft tissues, such as skeletal muscle. It is among the most common soft tissue sarcomas in late adulthood. It is much more aggressive than AFX, with higher recurrence and higher metastatic rates. MFHs are treated surgically with either WLE or MMS.
Epidemiology
Although MFHs occur at a rate of approximately 1.5 per million, they are the third most common cutaneous soft tissue sarcoma after Kaposi sarcoma and dermatofibrosarcoma protuberans. MFHs typically appear between the sixth and eighth decade of life, although childhood tumors have been reported. They are more common in whites and there is a slight male predominance (nearly 3:1). The head and neck are the most common locations for subcuticular MFHs followed closely by the extremities; tumors on upper extremities occur almost twice as often as those on the thighs or legs. Distal tumors have higher 5-year survival than proximal tumors.
Cause and Pathogenesis
Although originally believed to have a histiocytic origin, evidence suggests that MFHs develop from mesenchymal progenitor cells. The exact cause of MFH remains elusive; reports of MFH occurring at surgical sites, burn scars, areas of chronic inflammation, or internal fractures have led to the hypothesis that MFH is a reactive process occurring at sites of trauma. Ionizing radiation may also play a role in the development of this malignancy.
It is difficult to ascertain precise rates of recurrence and metastasis for subcutaneous MFH because most reports contain data that combine both subcutaneous and soft tissue MFH. Regardless of location, the tumor is biologically aggressive; recurrence and metastatic rates for both subcutaneous and deep MFHs are taken into account.
Up to 71% of MFHs have recurred after surgical treatment and the time to recurrence is usually within 2 years of treatment. A significant number of patients may develop either recurrence or metastases after 2 years, highlighting the necessity for close follow-up of these patients. Deep MFHs have a much higher risk for metastasis than their subcuticular counterpart. Metastasis has occurred in up to 44% of MFHs, but is reported to be as low as 17% of cases in subcuticular tumors. The most common location for metastasis is the lung, followed by regional nodal beds. Survival is based on tumor size with overall 5-year survival approximately 50%. Tumor size and high histologic grade seem to have the greatest effect on metastasis and survival. Despite the histologic grade, tumors less than 5 cm have approximately a 79% survival rate, whereas tumors between 5 and 10 cm and tumors greater than 10 cm have survival rates of 63% and 41%, respectively.
Because of the high metastatic potential of MFH, sentinel lymph node biopsy is recommended for all diagnosed cases. In addition, imaging is not only necessary to rule out metastatic disease at the time of diagnosis but also assists surgeons in planning the initial surgical margins.
Clinical Features
MFHs have a propensity to occur beneath the fascia, and subcutaneous or dermal tumors are less common. It most commonly presents as a deep painless enlarging mass with a rapid rate of growth ( Fig. 3 ). Superficial MFHs extend only down to fascia, whereas deep MFHs go below fascia to muscle and bone; most present as deep tumors. Although previously believed to occur most commonly on the extremities, the head and neck may be the most common location; it is vital to differentiate tumors occurring on the face from AFX. The retroperitoneum is also a common site of occurrence and presents with abdominal symptoms, and this presentation has the worst prognosis. MFHs spread considerably along fascial planes and between muscle fibers, causing difficulty in assessing the full extent of the tumor. The differential diagnosis includes, but is not restricted to, pleomorphic liposarcoma, rhabdomyosarcoma, AFX (when superficial), dermatofibrosarcoma protuberans, epithelioid sarcoma, and fibrosarcoma.
Diagnosis
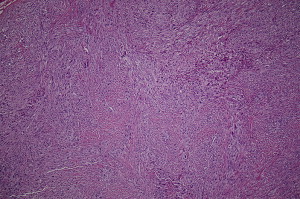
The diagnosis of MFH is difficult, and is frequently a diagnosis of exclusion because it shares many histologic similarities with an assortment of poorly differentiated tumors. Five subtypes have been described: storiform-pleomorphic (most common, Fig. 4 ), myxoid, giant cell, inflammatory, and angiomatoid. MFH looks similar to AFX, with the pleomorphic subtype at times being cellularly indistinguishable. This type contains plump pleomorphic spindle cells, numerous atypical mitoses, foam and giant cells, and marked pleomorphism (see Fig. 3 ). Angioinvasion is common. Location plays an important role in the diagnosis of pleomorphic MFH, as superficial tumors typically represent AFX.

Immunohistochemistry may aid in the diagnosis of MFH. Similar to AFX, MFHs stain positive for CD68, smooth muscle actin, and vimentin. α1-antitrypsin and α1-chemotrypsin staining typically displays a varying degree of positivity. The angiomatoid subtype may stain positive for factor VIII–related antigen and Ulex europaeus . S-100, HMB-45, CD34, cytokeratin, and desmin are negative. Having such similar histologic and immunologic characteristics as AFX, other immunostains may be useful in differentiating the two. LN-2(CD74) was shown to be expressed to a higher degree in MFH than AFX. As stated earlier, procollagen-1, CD99, CD117, and CD10 tend to show greater affinity for AFX. Molecular studies for mutations in the p53 gene have shown that AFXs have higher immunoreactivity for cyclobutane pyrimidine dimers; mutations in both K- ras and H- ras genes have been seen in MFH but not AFX. Furthermore, AFX shows a diploid distribution on flow cytometry, whereas MFH displays aneuploidy, although aneuploidy may be more of an indicator of malignant potential rather than an indicator of a specific tumor. These molecular findings may not only help to differentiate between AFX and MFH they may also shed light on the pathogenesis of these poorly understood tumors.
Treatment
The standard treatment of MFH is surgical resection, either with WLE, MMS, or amputation in extreme cases. As previously stated, before surgical planning, imaging is necessary to assist in determination of the surgical margins; magnetic resonance imaging (MRI) is more sensitive than computed tomography (CT) for soft tissue detail.
Clearance rates with WLE have been disappointing, with reported recurrence rates of 17% to 71%. This can be attributed to the highly infiltrative growth pattern displayed by MFH, with tumor radiating many centimeters from the clinically apparent mass. As many as half of excised tumors may have positive margins that require at least 1 reexcision to achieve negative pathologic margins. Definite parameters have not been set with regard to the surgical margin, but at least a 2-cm margin should be taken from the lateral extent of the tumor unless otherwise directed by MRI/CT. Excisions should be carried to and include the fascia for subcutaneous MFH, and for deeper soft tissue MFH excisions may need to involve bone for tumor clearance.
As previously stated, MFHs that occur in the subcutis have a propensity for growth well beyond the tumor mass, making margin control paramount with resection of the tumor. It would make sense then that MMS would be to the patient’s advantage in initial clearance of this tumor. MMS has been used sparsely for the treatment of MFH, but it has been shown to be extremely promising as a therapeutic modality. Of 28 cases of MFH reported to have been treated with MMS, there were only 5 recurrences, yielding a clearance rate of 82%. Follow-up for these tumors was short, averaging about 2.4 years. MMS allows for immediate evaluation of the entire surgical margin and is not only superior to traditional WLE with regard to clearance of subcuticular MFH it also offers tissue conservation for improved cosmesis. For MFH involving deeper structures, it is unlikely that a Mohs surgeon would perform the primary resection. However, when available a Mohs surgeon would be useful to evaluate the tissue specimen using Mohs histologic techniques to ensure that the entire surgical margin is evaluated. This may provide a higher immediate cure rate and fewer potential surgeries and subsequent exposure to general anesthesia for the patient. Chemotherapy and surgery may also improve long-term survival.
MFH
History
MFH was first described in 1961 by Kauffman and Stout; previously, it had been referred to by such names as fibroxanthoma, malignant fibrous xanthoma, malignant giant tumor of soft parts, and pleomorphic fibrosarcoma. MFH is best regarded as a soft tissue sarcoma and is now referred to by many as pleomorphic sarcoma. The questions surrounding its origin and its many subtypes have made the diagnosis of MFH as its own entity controversial. Although MFHs arise in subcutaneous tissue, they arise more commonly in soft tissues, such as skeletal muscle. It is among the most common soft tissue sarcomas in late adulthood. It is much more aggressive than AFX, with higher recurrence and higher metastatic rates. MFHs are treated surgically with either WLE or MMS.
Epidemiology
Although MFHs occur at a rate of approximately 1.5 per million, they are the third most common cutaneous soft tissue sarcoma after Kaposi sarcoma and dermatofibrosarcoma protuberans. MFHs typically appear between the sixth and eighth decade of life, although childhood tumors have been reported. They are more common in whites and there is a slight male predominance (nearly 3:1). The head and neck are the most common locations for subcuticular MFHs followed closely by the extremities; tumors on upper extremities occur almost twice as often as those on the thighs or legs. Distal tumors have higher 5-year survival than proximal tumors.
Cause and Pathogenesis
Although originally believed to have a histiocytic origin, evidence suggests that MFHs develop from mesenchymal progenitor cells. The exact cause of MFH remains elusive; reports of MFH occurring at surgical sites, burn scars, areas of chronic inflammation, or internal fractures have led to the hypothesis that MFH is a reactive process occurring at sites of trauma. Ionizing radiation may also play a role in the development of this malignancy.
It is difficult to ascertain precise rates of recurrence and metastasis for subcutaneous MFH because most reports contain data that combine both subcutaneous and soft tissue MFH. Regardless of location, the tumor is biologically aggressive; recurrence and metastatic rates for both subcutaneous and deep MFHs are taken into account.
Up to 71% of MFHs have recurred after surgical treatment and the time to recurrence is usually within 2 years of treatment. A significant number of patients may develop either recurrence or metastases after 2 years, highlighting the necessity for close follow-up of these patients. Deep MFHs have a much higher risk for metastasis than their subcuticular counterpart. Metastasis has occurred in up to 44% of MFHs, but is reported to be as low as 17% of cases in subcuticular tumors. The most common location for metastasis is the lung, followed by regional nodal beds. Survival is based on tumor size with overall 5-year survival approximately 50%. Tumor size and high histologic grade seem to have the greatest effect on metastasis and survival. Despite the histologic grade, tumors less than 5 cm have approximately a 79% survival rate, whereas tumors between 5 and 10 cm and tumors greater than 10 cm have survival rates of 63% and 41%, respectively.
Because of the high metastatic potential of MFH, sentinel lymph node biopsy is recommended for all diagnosed cases. In addition, imaging is not only necessary to rule out metastatic disease at the time of diagnosis but also assists surgeons in planning the initial surgical margins.
Clinical Features
MFHs have a propensity to occur beneath the fascia, and subcutaneous or dermal tumors are less common. It most commonly presents as a deep painless enlarging mass with a rapid rate of growth ( Fig. 3 ). Superficial MFHs extend only down to fascia, whereas deep MFHs go below fascia to muscle and bone; most present as deep tumors. Although previously believed to occur most commonly on the extremities, the head and neck may be the most common location; it is vital to differentiate tumors occurring on the face from AFX. The retroperitoneum is also a common site of occurrence and presents with abdominal symptoms, and this presentation has the worst prognosis. MFHs spread considerably along fascial planes and between muscle fibers, causing difficulty in assessing the full extent of the tumor. The differential diagnosis includes, but is not restricted to, pleomorphic liposarcoma, rhabdomyosarcoma, AFX (when superficial), dermatofibrosarcoma protuberans, epithelioid sarcoma, and fibrosarcoma.
Diagnosis
The diagnosis of MFH is difficult, and is frequently a diagnosis of exclusion because it shares many histologic similarities with an assortment of poorly differentiated tumors. Five subtypes have been described: storiform-pleomorphic (most common, Fig. 4 ), myxoid, giant cell, inflammatory, and angiomatoid. MFH looks similar to AFX, with the pleomorphic subtype at times being cellularly indistinguishable. This type contains plump pleomorphic spindle cells, numerous atypical mitoses, foam and giant cells, and marked pleomorphism (see Fig. 3 ). Angioinvasion is common. Location plays an important role in the diagnosis of pleomorphic MFH, as superficial tumors typically represent AFX.
Immunohistochemistry may aid in the diagnosis of MFH. Similar to AFX, MFHs stain positive for CD68, smooth muscle actin, and vimentin. α1-antitrypsin and α1-chemotrypsin staining typically displays a varying degree of positivity. The angiomatoid subtype may stain positive for factor VIII–related antigen and Ulex europaeus . S-100, HMB-45, CD34, cytokeratin, and desmin are negative. Having such similar histologic and immunologic characteristics as AFX, other immunostains may be useful in differentiating the two. LN-2(CD74) was shown to be expressed to a higher degree in MFH than AFX. As stated earlier, procollagen-1, CD99, CD117, and CD10 tend to show greater affinity for AFX. Molecular studies for mutations in the p53 gene have shown that AFXs have higher immunoreactivity for cyclobutane pyrimidine dimers; mutations in both K- ras and H- ras genes have been seen in MFH but not AFX. Furthermore, AFX shows a diploid distribution on flow cytometry, whereas MFH displays aneuploidy, although aneuploidy may be more of an indicator of malignant potential rather than an indicator of a specific tumor. These molecular findings may not only help to differentiate between AFX and MFH they may also shed light on the pathogenesis of these poorly understood tumors.
Treatment
The standard treatment of MFH is surgical resection, either with WLE, MMS, or amputation in extreme cases. As previously stated, before surgical planning, imaging is necessary to assist in determination of the surgical margins; magnetic resonance imaging (MRI) is more sensitive than computed tomography (CT) for soft tissue detail.
Clearance rates with WLE have been disappointing, with reported recurrence rates of 17% to 71%. This can be attributed to the highly infiltrative growth pattern displayed by MFH, with tumor radiating many centimeters from the clinically apparent mass. As many as half of excised tumors may have positive margins that require at least 1 reexcision to achieve negative pathologic margins. Definite parameters have not been set with regard to the surgical margin, but at least a 2-cm margin should be taken from the lateral extent of the tumor unless otherwise directed by MRI/CT. Excisions should be carried to and include the fascia for subcutaneous MFH, and for deeper soft tissue MFH excisions may need to involve bone for tumor clearance.
As previously stated, MFHs that occur in the subcutis have a propensity for growth well beyond the tumor mass, making margin control paramount with resection of the tumor. It would make sense then that MMS would be to the patient’s advantage in initial clearance of this tumor. MMS has been used sparsely for the treatment of MFH, but it has been shown to be extremely promising as a therapeutic modality. Of 28 cases of MFH reported to have been treated with MMS, there were only 5 recurrences, yielding a clearance rate of 82%. Follow-up for these tumors was short, averaging about 2.4 years. MMS allows for immediate evaluation of the entire surgical margin and is not only superior to traditional WLE with regard to clearance of subcuticular MFH it also offers tissue conservation for improved cosmesis. For MFH involving deeper structures, it is unlikely that a Mohs surgeon would perform the primary resection. However, when available a Mohs surgeon would be useful to evaluate the tissue specimen using Mohs histologic techniques to ensure that the entire surgical margin is evaluated. This may provide a higher immediate cure rate and fewer potential surgeries and subsequent exposure to general anesthesia for the patient. Chemotherapy and surgery may also improve long-term survival.
Sebaceous carcinoma
History
Carcinoma of the meibomian gland was first reported in the literature in the late nineteenth century, though sebaceous carcinoma was not classified as a unique type of cutaneous cancer until the early twentieth century. Advancements in understanding of the natural history and clinical presentation of sebaceous carcinoma, particularly carcinomas appearing in the eyelid, were then described in several case series throughout the middle twentieth century. In recent decades, studies have attempted to further elucidate the epidemiologic and pathologic characteristics of the disease. In addition, research has explored the effectiveness of various treatment options.
Epidemiology
Sebaceous carcinoma is a rare cutaneous tumor arising from the sebaceous glands. Between 1973 and 2004, 1349 cases were identified and reported to the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) database. Sebaceous carcinoma accounts for 0.2% to 5.5% of the cutaneous malignancies occurring on the eyelid. The SEER study also indicates a yearly incidence of 2.3 cases per million in whites, 1.07 per million in Asian/Pacific Islanders, and 0.48 per million in blacks. Most patients with sebaceous carcinoma are more than 50 years of age (most commonly between ages 60 and 80 years) and most are white. Furthermore, women have often been labeled as high risk for developing sebaceous carcinoma, but more recent population-wide studies have shown a lack of association between gender and development of the disease.
Cause and Pathogenesis
The cause of most sebaceous carcinomas is unknown. Most cases arise de novo, and not from a preexisting sebaceous condition, although some cases have been associated with immunosuppression or previous radiation to the tumor site. Significant associations with Muir-Torre syndrome have been identified. Because sebaceous carcinomas occur most commonly around the eye, the tumors types are traditionally divided into 2 categories: ocular and extraocular.
Clinical Features
Most cases of sebaceous carcinoma appear on the head or neck, with up to 75% of cases occurring on the eyelid. Ocular sebaceous carcinomas typically present as a small, slowly growing, single papule or nodule on the eyelid. These papules closely resemble chalazia and tend to occur on the upper eyelid, as more meibomian glands and glands of Zeis are located on the upper lid. The eyelid may also swell diffusely, resembling inflammatory processes such as blepharitis or cicatricial pemphigoid. In addition, the eyelid tissue may be distorted, thus preventing the eyelids from closing. If there is advanced pagetoid spread, the carcinoma may present with eyelash loss, lid eversion or undulation, ocular distortion, and erosion and ulceration.
Extraocular sebaceous carcinoma usually appears as a firm yellow-hued papule (see Fig. 4 ); ulceration may be present. Although other sites may be involved, extraocular tumors are most commonly seen on the head and neck. Ocular sebaceous carcinomas share many clinical features with other eyelid lesions, often leading to a delay in proper diagnosis. Most commonly, sebaceous carcinoma is mistaken for chalazion and blepharoconjuctivitis. Sebaceous carcinoma may also resemble 3 more common malignancies of the eyelid: basal or squamous cell carcinoma and malignant melanoma. Differential diagnosis of sebaceous carcinoma also includes the following: keratoconjunctivitis, unilateral conjunctivitis, cutaneous horn, ocular pemphigoid, leukoplakia, conjunctival carcinoma in situ, granulomatous inflammation, central retinal artery occlusion and proptosis, lacrimal gland tumors, exophthalmos, pyogenic granulomas, metastatic tumors, Merkel cell carcinoma, sarcoidosis, meibomitis, clear-cell eccrine hidradenoma, and benign adnexal tumors.
As mentioned previously, sebaceous carcinoma is associated with Muir-Torre syndrome and is considered a marker for this disease. Sebaceous adenomas and epitheliomas related to this syndrome also tend to appear on the face and may occur as single or multiple papules. They are skin-colored, yellowish, or reddish-brown, and are occasionally ulcerated papules. These tumors may resemble sebaceous hyperplasia. Keratoacanthoma, squamous cell carcinoma, and multiple follicular cysts may also occur as part of this syndrome.
Both ocular and extraocular sebaceous carcinomas have been known to metastasize to regional lymph nodes; preauricular and parotid nodes are the most common sites of metastasis. Less frequently, they may also metastasize to distant sites such as the liver, lungs, brain, and bones. In addition, sebaceous carcinoma is associated with secondary malignancies commonly seen with Muir-Torre syndrome, such as colorectal and genitourinary tumors.
Diagnosis
Because it mimics a variety of other cutaneous malignancies, identification of sebaceous carcinoma can be problematic. Diagnosis of the disease is often delayed by its clinical and histologic ambiguity, leading to improper treatment as well as increased morbidity and mortality. Therefore, particular attention should be paid to suspicious chalazia and inflammations that fail to respond to appropriate treatment. Biopsies of potential sebaceous carcinomas, coupled with vigilant histologic examination, are crucial components to proper diagnosis.
In addition to its ambiguous clinical presentation, sebaceous carcinoma also mimics a myriad of malignancies histologically. Sebaceous carcinomas are centered in the dermis and consist of aggregations of neoplastic cells. The tumors may be classified as well, moderately, or poorly differentiated, and most often present as irregular, lobular sebaceous growths. The nuclei are commonly pleomorphic, and the cells typically exhibit increased mitotic activity, basaloid features, and hyperchromatic nuclei. The undifferentiated, neoplastic cells usually present with foamy cytoplasm because of an abundance of small lipid globules ( Fig. 5 ). Vacuolization of the cytoplasm of moderately differentiated or well-differentiated cells may indicate sebaceous carcinoma, and sebaceous carcinoma tumors often have areas of central necrosis, similar to the pattern of comedocarcinoma. The classic identifier of sebaceous carcinoma, however, is intraepithelial spread beyond the main site of the tumor into the conjunctival epithelium and the epidermis of the eyelid. This pagetoid growth pattern may appear similar to Bowenoid actinic keratosis in the eyelid and carcinoma in situ in the conjunctiva. Moreover, vacuolated sebaceous carcinoma cells show abundant lipid content if stained with Oil Red O and Sudan IV stains.
Related posts:
 Mohs Micrographic Surgery Technique
Mohs Micrographic Surgery Technique
 Mohs Surgery for Squamous Cell Carcinoma
Mohs Surgery for Squamous Cell Carcinoma
 Flaps and Grafts Reconstruction
Flaps and Grafts Reconstruction
 Management of Skin Cancer in Solid-organ Transplant Recipients: A Multidisciplinary Approach
Special Considerations for Mohs Micrographic Surgery on the Eyelids, Lips, Genitalia, and Nail Unit
Multidisciplinary Approach to Large Cutaneous Tumors of the Head and Neck
Management of Skin Cancer in Solid-organ Transplant Recipients: A Multidisciplinary Approach
Special Considerations for Mohs Micrographic Surgery on the Eyelids, Lips, Genitalia, and Nail Unit
Multidisciplinary Approach to Large Cutaneous Tumors of the Head and Neck
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


