Introduction
Millions of people across the globe suffer from disfiguring traumatic and burn scars with far-reaching physical, psychological, and social impacts. The scars may result in profound functional limitations, disfigurement, symptoms, and emotional distress, severely degrading overall quality of life. Though readers of this text often have the requisite skills and tools available to assist these patients, issues such as lack of awareness, nonintersecting practice patterns, and underdeveloped reimbursement schemes may keep the patients largely out of sight.
In contrast to surgical scars for which procedures are often meticulously planned and performed to camouflage associated scars, traumatic and burn scars are inherently heterogenous and often follow a prolonged time course owing to factors such as the variability and unplanned nature of the insult, potential high-energy mechanisms, and relatively large areas of involvement. Differences in access to posttrauma care adds to the variability in outcomes worldwide. Additionally, there may be injuries to deeper structures such as nerves, vessels, bones, muscles, and fascia that may have a significant impact on ultimate function and appearance.
The presentation of a patient after traumatic injury often includes both the sequelae of primary injury as well as changes due to surgical management (e.g., split- and full-thickness skin grafting, tissue rearrangement, biological implants, etc.) and any downstream revisions. Given the protean nature of traumatic scars, management often poses significant challenges requiring a multidisciplinary approach that may include dermatologic surgeons, surgical specialists (e.g., burn, plastics, orthopedics, etc.), physical and occupational therapists, psychologists, case managers, and others. Furthermore, it is imperative that the treatment approach remains adaptable and incorporates multiple modalities and longitudinal follow-up to achieve the best possible outcomes.
This chapter provides a synthesis of the characteristics and management of traumatic and burn scars from a dermatologic surgery perspective with an emphasis on minimally invasive techniques such as lasers. Although traumatic scars are often complex, readers should not be needlessly intimidated out of an extremely rewarding and underappreciated aspect of practice. The reader will gain an understanding of the pathophysiology, classification, assessment, and treatment modalities for these types of scars. This chapter aims to equip readers with the knowledge necessary to begin their journey toward improving the lives of patients and enhancing practice satisfaction.
Epidemiology
Traumatic scars represent a significant global health care burden with a wide-ranging impact on individuals and communities. In the United States, for example, it is estimated that approximately 100 million people experience traumatic injuries annually; a considerable proportion of these injuries result in visible and symptomatic scarring. Burn injuries also contribute significantly to the prevalence of scars, with approximately 1.25 million individuals receiving treatment for burns each year and around 50,000 of these cases requiring hospitalization.
The incidence and prevalence of traumatic and burn scars vary depending on numerous factors such as geographical location, socioeconomic status, and cultural practices. In high-income countries, traumatic scars often result from motor vehicle accidents, falls, and interpersonal violence. In low- and middle-income countries, they are more commonly associated with occupational injuries, conflict-related incidents, and domestic accidents. Burns are influenced by factors such as access to safe cooking and heating facilities, fire safety measures, and awareness of burn prevention strategies. Limited access to proper initial wound management and ongoing follow-up may also contribute to a higher prevalence of pathologic scars following traumatic injuries or burns in low-income countries.
Mechanisms of Injury
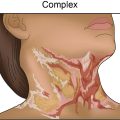
Understanding the location and mechanism of injury and postinjury course is crucial when assessing a traumatic or burn scar. Heterogenous mechanisms, variable management, and timing after injury influence the ultimate presentation including scar thickness, color, texture, symptoms, and overall impact on quality of life at a particular point in time. Within weeks after injury, patchy erythema may herald incipient pathological scars and contractures that may develop only after several months. The development of pathological scarring (e.g., hypertrophic scars and keloids) is heavily influenced by the depth of dermal injury. For example, a scald injury with boiling water might result in hypertrophic scarring centrally while more superficial injury at the periphery results only in dyspigmentation. Lacerations also provide a good example of the influence of depth—a single linear cut may include both normotrophic and hypertrophic portions based in part on the depth of injury and the different populations of fibroblasts impacted (see Fig. 10.1 ). Penetrating trauma resulting from knife or gunshot wounds may produce scars that appear relatively small clinically but may be associated with injury to deeper structures, tethering, and through-and-through injuries that result in profound symptoms and disability. Patient factors unrelated to the initial injury may also influence the incidence of pathological scarring. For example, persistent inflammation induced by tension (e.g., location on chest and upper back, across a joint, etc.), hair follicles impacted by scarring (e.g., bundled and trapped hairs), or bacterial/fungal infection and colonization may exacerbate scarring.

Blast injuries incorporate thermal, crush, and sheer forces that can result in broad scars, volume loss, amputation, and traumatic tattooing with organic and inorganic contaminants. Furthermore, traumatic brain injury that accompanies blasts and other major trauma may result in invisible scars that complicate overall recovery. Burns can result from thermal, chemical, or electrical mechanisms and can affect large body surface areas and perhaps unseen structures with profound effects on cosmesis and function. Unsurprisingly, pathologic scarring more commonly affects contaminated blast wounds or burn injuries than clean surgical procedures. Ninety-one percent of burn wounds may be complicated by hypertrophic scarring that can contribute to disability and intense pruritus.
Injury mechanism may also impact patient perception of scarring and the psychological aspects surrounding trauma recovery. For example, symptoms of posttraumatic stress may be induced by the sights, smells, sensations, and anxiety that accompany procedural scar management. Perceptions about particular scars may also be nuanced. For example, a scar might be a positive badge of honor reflecting bravery and camaraderie. Or for some, it could be a source of disability with a constant negative reminder of trauma and loss. Visible scars, such as those on the face, may induce negative reactions in others that in turn impact the perception of the patient. By considering the specific injury mechanism, clinical presentation, and the patient’s response to the scarring, providers can tailor the management approach to the patient’s needs and goals at a particular time.
Burn Wound Pathophysiology
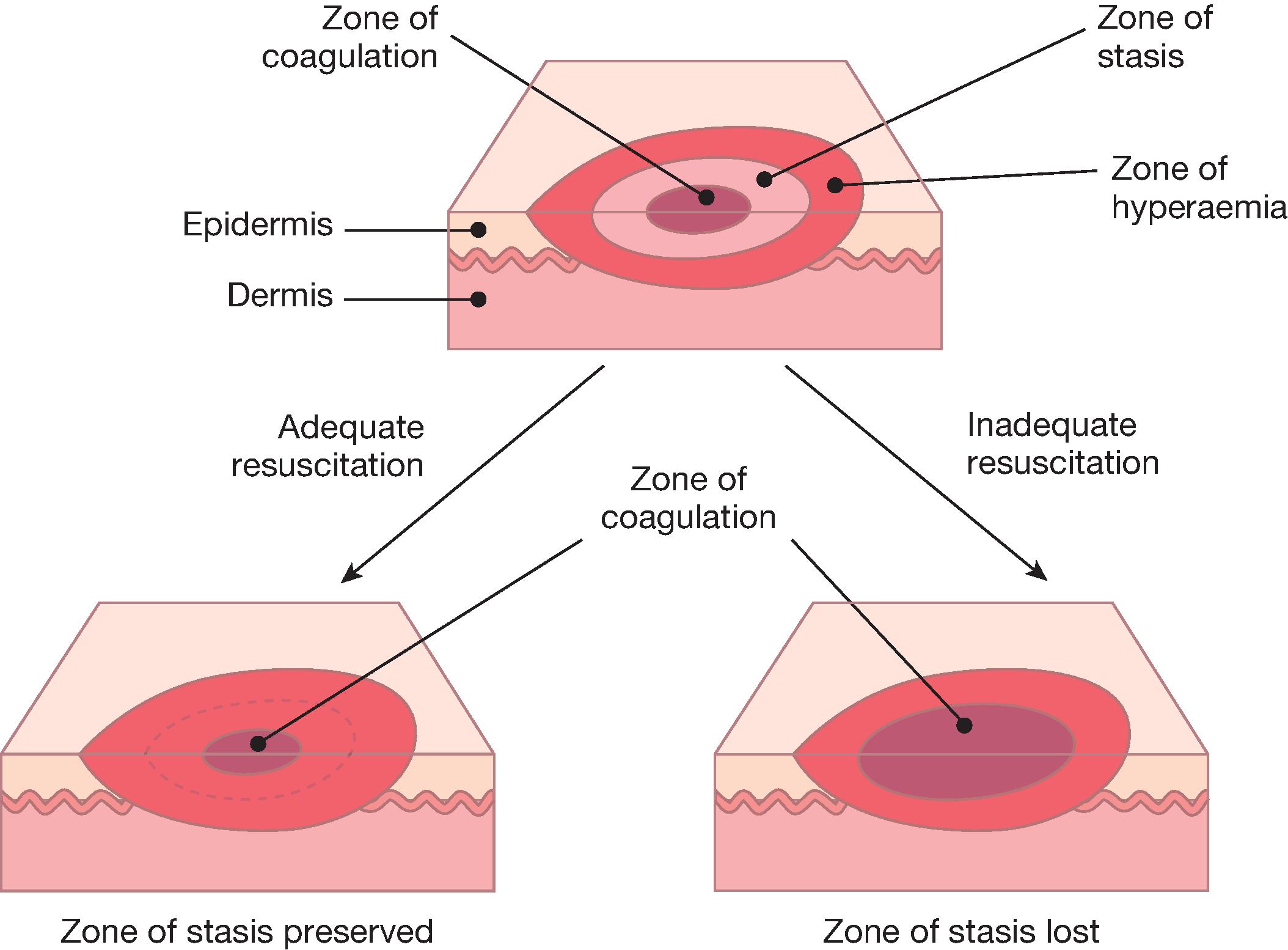
The prevalence of burns and their unique characteristics merit some distinction from the overall umbrella of traumatic scars. A basic understanding of burn injury responses is essential to anticipate the expected course and identify key points of intervention. Jackson’s burn theory describes three concentric zones of potential tissue viability radiating out from the center of the injury toward the periphery; the relative size of the zones of coagulation, stasis, and hyperemia are determined by the temperature (or concentration, etc.) and duration of exposure (see Fig. 10.2 ). The zone of coagulation adjacent to the burn source is associated with irreversible tissue necrosis and is a driver of pathological scar formation. Cellular disruption and damage to the extracellular matrix trigger inflammation that produces edema and ischemia in the surrounding zone of stasis. Tissue in this zone is potentially viable if the ischemia can be mitigated. The outer zone of hyperemia is a vascular response to injury that facilitates the healing process. Correctly identifying these zones can help optimize postburn care (e.g., necrotic tissue should ideally be debrided without removing potentially viable tissue). In the acute phase of burn management, fluid resuscitation aims to maintain perfusion of vital organs while correcting for incidental losses and fluid shifts. However, excessive fluid can exacerbate secondary edema and contribute to expansion of the zone of stasis. Relative hypoxia in this zone can enlarge the zone of necrosis and, ultimately, the resulting scar. Judicious fluid resuscitation to achieve systemic targets but also limit expansion of the zone of stasis is crucial to limit further necrosis and incipient scar formation.
Features of Traumatic and Burn Scars
Traumatic and burn scars exhibit features that distinguish them from scars of other origin. Each traumatic scar has a unique presentation based on the circumstances of the injury (e.g., location, duration, mode, timing, etc.), patient characteristics (e.g., age, skin type, access to care, etc.), and subsequent management. There is no one single therapeutic intervention for all “traumatic” scars, since they will vary considerably in terms of erythema, hyperpigmentation, hypopigmentation, atrophy, hypertrophy, pliability, symptoms, and degree of contracture. A single injury site may exhibit portions with all these features. Contractures adjacent to joints or free edges may also be associated with significant disability and disfigurement. The impact of traumatic scars in children may vary and accumulate over time based on ongoing growth and development. Following burns and other sources of trauma, consideration should be given to prior treatments, future surgical interventions, prosthetic use, sensitivities and pain syndromes, and presence of mental health impacts like posttraumatic stress.
Appearance
Owing to the nature of the injury, traumatic scars may be associated with irregular borders, tissue loss, and the involvement of multiple cosmetic subunits, making them challenging to manage functionally and cosmetically. Additionally, they can be associated with damage to deeper tissues including muscles, nerves, bones, blood vessels, and lymphatics, potentially leading to functional impairments beyond the impact of the scarred skin. Burn scars can exhibit unique characteristics based on the depth of the injury. Superficial burns, such as first-degree burns, may result only in temporary erythema, dyspigmentation, and mild scarring. Deeper burns, including second-degree and third-degree burns, are frequently associated with more severe and longer-lasting scars (e.g., pathological scars including hypertrophic scars and keloids). These scars can be thick and raised and may limit joint mobility. The appearance of hypertrophic scars, keloids, and related contractures may be delayed several months after an injury; prolonged erythema can be a harbinger of incipient pathological scars and merits consideration for early procedural intervention. Distinguishing hypertrophic scars and keloids can be difficult initially based only on clinical appearance. Clues such as a history of prior keloids, scars that extend beyond the borders of the original injury, or scars that are more refractory to treatment may indicate the presence of keloids.
Pain and Itch
Chronic pain and itch often accompany hypertrophic scars and keloids, profoundly impacting both the physical and psychological well-being of affected patients. The sensation, perception, and management of pain and itch are complex, and a full discussion is beyond the scope of this chapter. Neuropathic pain is caused by a lesion or disease of the somatosensory nervous system, such as the sequelae of traumatic injuries. Descriptions of pain are divided into positive (e.g., heightened and/or abnormal sensations) and negative (e.g., diminished sensation) symptoms. Multiple mechanisms may be involved in neuropathic pain and therefore multimodal treatment may be required. Chronic pruritus can be all-consuming for patients; compulsive scratching can become a maladaptive habit and lead to a self-reinforcing pattern of scratching, further tissue damage, and worsening itch. The traditional management of chronic, moderate-to-severe pain and itch may include an ascending ladder of topical (e.g., local anesthetics, doxepin, etc.), injected/intralesional (e.g., steroids, nerve blocks, etc.), and systemic medications (e.g., gabapentin, tricyclic antidepressants, etc.), as well as physical and behavioral therapy. Energy-based devices are a novel and underrecognized therapy for scar-related pain and itch and potentially potent complement to standard therapy. They will be discussed later in the chapter.
Contractures
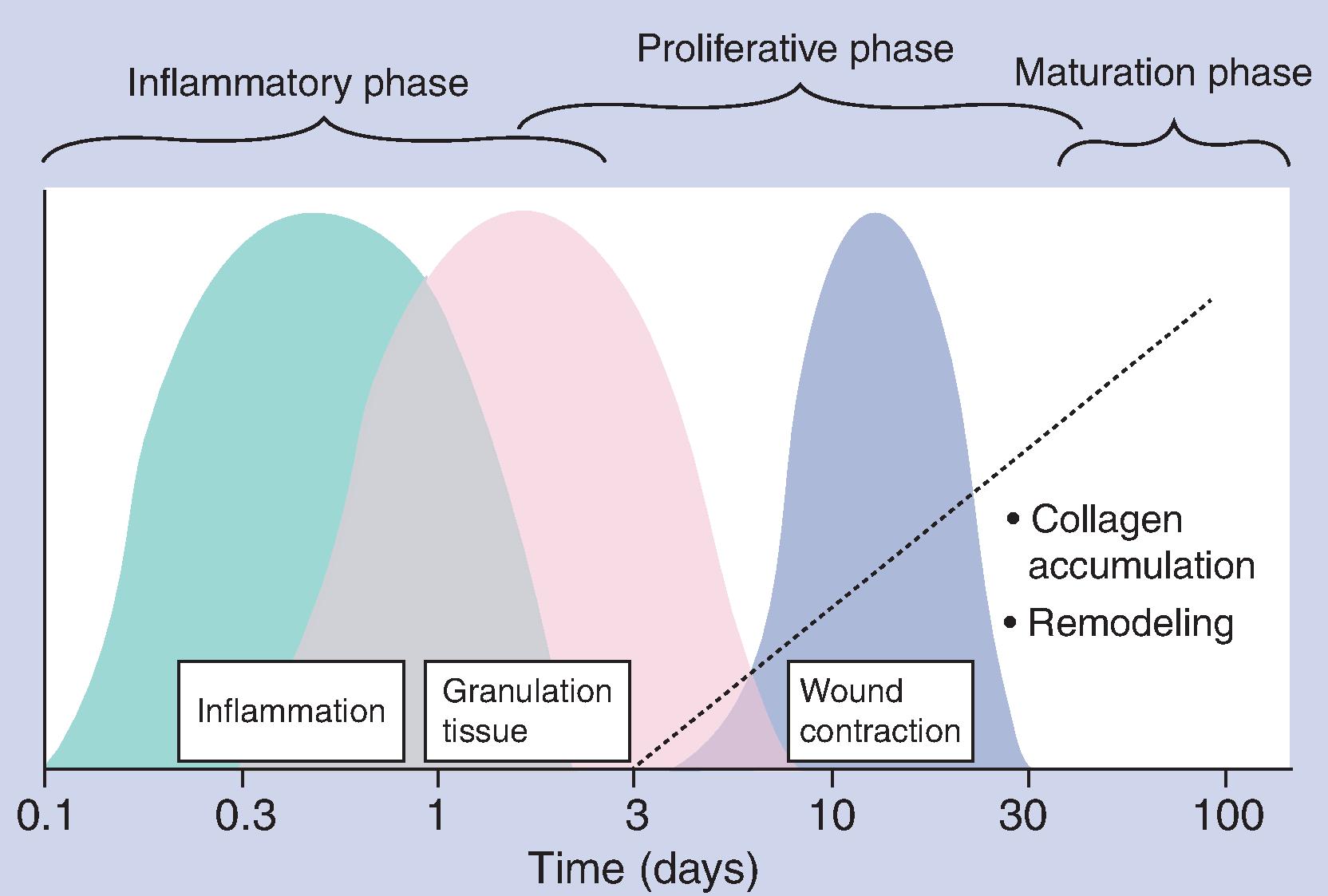
The three phases of wound healing—inflammation, proliferation, and remodeling—have been well described in the literature (see Fig. 10.3 ). Scar contraction is a predictable consequence of the remodeling phase of healing that occurs in the transition from proliferation to remodeling approximately 3 weeks to 2 years after injury. Contractures frequently complicate recovery after traumatic injury, especially when the scars cross joints or are close to free margins (e.g., eyelid, lip). In the absence of adequate immediate (e.g., surgical reconstruction, tissue replacement, treatment of infections, etc.) and long-term (e.g., physical and occupational therapy, surgical revision, etc.) postinjury care, catastrophic contractures can develop in areas such as the hand, neck, elbow, knee, and ankle (see Fig. 10.4 ). Decreased range of motion and functional impairment can be devastating to patients and families with potential loss of employment and developmental issues in children.

Adnexal Structures
Adnexal structures, including hair follicles, eccrine glands, and sebaceous glands, play a crucial role in the normal functioning and appearance of healthy skin. Scar tissue is characterized by a near total loss of adnexal structures that contribute to permanent changes in appearance (e.g., alopecia), disordered function (e.g., inability to sweat), and skin fragility with compromised healing. Normal wound healing involves stem cells residing in adjacent adnexal structures. Large areas of scar tissue are essentially deserts of tissue regeneration that must be recognized when considering therapeutic options.
Hair
Loss of hair follicles can be particularly noticeable in areas with abundant hair growth, leading to a stark contrast between the scar and the surrounding hair-bearing skin. Symptoms such as irritation, folliculitis, and abscesses may develop in scar tissue due in part to the entrapment of residual follicles. Persistent related inflammation can also be a driver of pathological scars. In addition, reconstructive procedures may relocate hair to areas not normally associated with hair growth (e.g., palms, inside the mouth). Hair on residual limbs requiring prosthetics may also be a source of persistent irritation and inflammation.
Eccrine Glands
Both excessive sweating (e.g., associated with prosthetic use) and the inability to sweat (associated with extensive traumatic scarring) are potentially important issues for many trauma and burn patients. Anhidrosis due to traumatic disruption of eccrine glands and ducts can contribute to temperature dysregulation that can negatively impact job performance and exercise tolerance. Disruption or entrapment of the eccrine apparatus may also result in pain and pruritus. Excessive sweating can lead to tissue maceration and a predilection for bacterial and fungal infections.
Sebaceous Glands
Sebaceous glands are responsible for producing sebum, which helps moisturize the skin and maintain its elasticity. In scars, reduced sebum production can result in dryness and increased susceptibility to cracking and flaking. The scar tissue may appear dry, rough, and less pliable compared to surrounding healthy skin.
Traumatic Tattoo
Explosive devises and various accidents can trap dirt, asphalt, shrapnel, and other contaminants in a wound. Just as scars can be a visible and permanent reminder of negative events, traumatic tattoos can be even more obvious because of the contrast with the normal skin color.
Volume Deficits and Contour Irregularities
In addition to scar formation, trauma can result in soft tissue or bony loss that may result in uneven or distorted surface topography. This may be further exacerbated by uneven wound healing, scar contraction, or uneven distribution of scar tissue.
Sequelae of Amputation
Limb amputation is relatively common among trauma patients and can predispose patients to a range of potential sequelae affecting the skin on the residual limb. The skin of the residual limb was not designed to accommodate weight bearing or the chronic occlusive and frictional forces associated with prosthetic use. The occlusive nature of a prosthetic sleeve coupled with constant friction and sweat accumulation can result in abrasions and folliculitis. These factors also predispose patients to infection (bacterial folliculitis and furuncle/carbuncle formation) and pain and ultimately may lead to time out of their prosthesis to allow for healing. These symptoms may be exacerbated by problematic hair and hyperhidrosis affecting the residual limb. In addition, the residual limb may be affected by pain issues such as heightened sensitivity and phantom limb pain, which should be considered when developing a therapeutic plan.
Scar Assessment
Scar assessment is an essential component of developing a treatment plan, evaluating the efficacy of various interventions, determining future management decisions, performing research, and obtaining documentation for reimbursement. More detailed and comprehensive assessments are generally required for scar-related research. Although many clinicians may not be involved in formal scar research, the outcome measures selected by researchers can play a large role in patient access for relatively new procedures such as laser scar management. The components of scar assessment include published and validated scar scales (e.g., Vancouver Scar Scale [VSS], Patient and Observer Scar Assessment Scale, etc.); patient-reported outcomes and quality-of-life assessments (e.g., SF-36, Burn-Specific Health Scale, etc.); and instruments for objective measurements including color, surface area, depth/height, and pliability. Direct measurements of degrees of range of motion and performance on functional assessments are especially valuable in the presence of scar contractures.
There are over a dozen published and validated scar scales, but the ideal scale does not yet exist. In particular, they fall short in adequately capturing the unique characteristics and complexities associated with traumatic and burn scars (see Tables 10.1 and 10.2 ). For example, one of the most used scales is the VSS that assesses scar pigmentation, vascularity, pliability, and height. Although simple and reproducible, its reliance on visual characteristics, lack of incorporation of symptoms and quality-of-life information, and lack of attention to function make it inadequate to capture the therapeutic potential of newer treatments such as ablative fractional resurfacing for traumatic scars. Since visual characteristics are only a surrogate for function and quality of life, future studies that rely exclusively on them will not necessarily contribute significantly to improved patient access despite positive outcomes.
| VSS | Modified VSS | Seattle Scale | MSS | Hamilton Scale | POSAS | Modified POSAS | MAPS | SBSES | UNC4P | VAS | DLQI | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Scar description | ||||||||||||
| Type | ||||||||||||
| Age | ||||||||||||
| Surface area | • | • | • | • | ||||||||
| Height/thickness/contour | • | • | • | • | • | • | • | • | • | |||
| Anatomic location | • | |||||||||||
| Erythema | • | • | • | • | ||||||||
| Pigmentation | • | • | • | • | • | • | • | • | • | |||
| Disruption of anatomic cosmetic units | ||||||||||||
| Scar comorbidities | ||||||||||||
| Psychosocial | • | |||||||||||
| Reaction of others | • | |||||||||||
| Hypertrichosis | ||||||||||||
| Hyperhidrosis/hypohidrosis | ||||||||||||
| Pain | • | • | • | • | • | • | ||||||
| Pruritus | • | • | • | • | • | |||||||
| Dysesthesia | • | • | ||||||||||
| Infection | ||||||||||||
| Lymphedema | ||||||||||||
| Chronic wound/ulceration | ||||||||||||
| Skin cancer | ||||||||||||
| Functional impairment | • | • | • | |||||||||
| Overall appearance, patient | • | • | ||||||||||
| Overall appearance, observer | • | • | • | |||||||||
| Amenability to treatment | ||||||||||||
| Validity | • | • | • | • | • | • | • | • |
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


