The preoperative assessment of the eye in facial paralysis is a critical component of surgical management. The degree of facial nerve paralysis, lacrimal secretion, corneal sensation, and lower eyelid position must be assessed accurately. Upper eyelid loading procedures are standard management of lagophthalmos. Lower eyelid tightening repositions the lower eyelid and helps maintain the aqueous tear film. Eyelid reanimation allows an aesthetic symmetry with blinking and restores protective functions vital to ocular preservation. Patients often have multiple nervous deficits, including corneal anesthesia. Other procedures include tarsorrhaphy, spring implantation, and temporalis muscle transposition; associated complications have rendered them nearly obsolete.
Key points
- •
Upper eyelid loading procedures are the gold standard for surgical management of lagophthalmos in the setting of a paralyzed upper eyelid.
- •
Lower eyelid tightening procedures reposition the lower eyelid and help to maintain the aqueous tear film of the eye.
- •
Lagophthalmos secondary to facial paralysis causes poor tear film movement and tear evaporation, which can lead to exposure keratitis, corneal abrasion, and permanent vision changes.
- •
Eyelid reanimation restores the protective functions vital to ocular preservation, which is particularly important because these patients often have multiple nervous deficits, including corneal anesthesia.
- •
Nonoperative management of patients with eyelid paralysis should be reserved for patients with reliable access to regular ophthalmologic examinations, overall good health, and minimal comorbidities.
Introduction
Facial paralysis has many devastating psychological, social, and physiologic consequences. Of the physiologic concerns, ocular preservation is the first and foremost priority in the management of the patient with facial paralysis. Medical and surgical interventions should be used as appropriate to ensure ocular safety and health. Appropriate patient education regarding the dangers of exposure keratitis is an important aspect of patient care. The management of the eye in facial paralysis may be led by the facial plastic surgeon, plastic surgeon, oculoplastic surgeon, or otolaryngologist, but early and effective communication and coordination of care between the patient, the ophthalmologist, and the surgeon managing the patient with facial paralysis is critical.
Upper eyelid loading for the treatment of paralytic lagophthalmos was first described in 1950 by Sheehan and popularized by Jobe in 1974. Lid loading procedures rely on gravitational forces to close the paralyzed upper eyelid by overcoming the action of the levator palpebrae superioris. Lower eyelid tightening is often implemented in conjunction with upper eyelid loading. As with all reanimation procedures in the paralyzed face, lid loading and lower eyelid tightening serve to restore the form and function of the paralyzed face. Eyelid reanimation can restore a static and dynamic symmetry to the eyes, but more importantly restores the protective functions that are vital to ocular preservation. These considerations are particularly important because these patients often have multiple cranial nerve deficits, such as corneal anesthesia and extraocular muscle paralysis. Other procedures for the paralyzed eyelids include tarsorrhaphy, spring implantation, and temporalis muscle transposition. However, their associated side effects and complications have left them with little, if any, indications for use today.
Introduction
Facial paralysis has many devastating psychological, social, and physiologic consequences. Of the physiologic concerns, ocular preservation is the first and foremost priority in the management of the patient with facial paralysis. Medical and surgical interventions should be used as appropriate to ensure ocular safety and health. Appropriate patient education regarding the dangers of exposure keratitis is an important aspect of patient care. The management of the eye in facial paralysis may be led by the facial plastic surgeon, plastic surgeon, oculoplastic surgeon, or otolaryngologist, but early and effective communication and coordination of care between the patient, the ophthalmologist, and the surgeon managing the patient with facial paralysis is critical.
Upper eyelid loading for the treatment of paralytic lagophthalmos was first described in 1950 by Sheehan and popularized by Jobe in 1974. Lid loading procedures rely on gravitational forces to close the paralyzed upper eyelid by overcoming the action of the levator palpebrae superioris. Lower eyelid tightening is often implemented in conjunction with upper eyelid loading. As with all reanimation procedures in the paralyzed face, lid loading and lower eyelid tightening serve to restore the form and function of the paralyzed face. Eyelid reanimation can restore a static and dynamic symmetry to the eyes, but more importantly restores the protective functions that are vital to ocular preservation. These considerations are particularly important because these patients often have multiple cranial nerve deficits, such as corneal anesthesia and extraocular muscle paralysis. Other procedures for the paralyzed eyelids include tarsorrhaphy, spring implantation, and temporalis muscle transposition. However, their associated side effects and complications have left them with little, if any, indications for use today.
Assessment of the eye in facial paralysis
The preoperative assessment of the facial paralysis patient is a critical component of their surgical management. The etiology and severity of the facial nerve paralysis must be accurately assessed before intervention. A detailed history of ocular issues before and since the onset of facial paralysis is an important part of the initial assessment. Preexisting ocular conditions, such as prior ophthalmologic surgery, chronic lid infections, ptosis, or refractive errors, may be exacerbated by the facial paralysis. Additionally, any and all prior interventions to manage the paralyzed eyelids must be documented. If the affected eye is the only seeing eye or the better seeing eye, then extra precautions must be taken ensure its health and safety. The physical examination of the patient with facial paralysis should include visual acuity, extraocular muscle assessment, visual fields, lacrimal secretion, corneal sensation, pupillary assessment, lower eyelid position, margin gap, and the presence or absence of a Bell’s phenomenon. Assessment of the marginal reflex distances 1 (MRD1) and 2 (MRD2) is also useful in assessing for ptosis and ectropion. The MRD1 is the distance from the pupillary light reflex to the upper eyelid. The MRD2 is the distance from the pupillary light reflex to the lower eyelid. The margin gap is the distance between the margin of the upper and lower eyelid with involuntary blink and maximal effort. The palpebral fissure height is the distance between the upper and lower eyelid in primary gaze. All patients with facial paralysis should be evaluated by an ophthalmologist to perform a baseline ophthalmologic examination and to establish care with an ophthalmologist ( Tables 1 and 2 ).
| History | Physical Examination |
|---|---|
| Comprehensive medical history | Comprehensive physical examination |
| Premorbid ocular symptoms | Eyebrow position |
| New ocular symptoms | Upper and lower eyelid position |
| Prior ophthalmologic surgery | Extraocular muscle movements |
| Prior facial reanimation surgery | Margin gap with blink and maximal effort |
| Marginal reflex distance (MRD); MRD1, MRD2 | |
| Palpebral fissure height | |
| Corneal sensation | |
| Pupillary assessment | |
| Bell’s phenomenon | |
| Fundoscopy |
| Test | Purpose |
|---|---|
| Visual acuity | Baseline visual acuity |
| Slit-lamp examination | Assess cornea, eyelids, conjunctiva, sclera, iris |
| Schirmer’s test | Assess aqueous tear production |
| Jones test | Assessment of physiologic nasolacrimal drainage |
| Visual fields | Visual field limitations |
Patients may present with good eye closure, but a poor blink response. These patients remain at risk for keratitis, owing to a loss of the windshield wiper effect of the blink with subsequent poor wetting of the cornea. Other patients may present with good eye closure while upright, but poor eye closure when supine. Although these patients seem to have good eye closure, consideration should be made for supplemental ocular lubrication, moisture chamber, or nighttime taping, if not surgical intervention. The presence or absence of a Bell’s phenomenon should also be noted. These patients are better able to tolerate poor eye closure because the cornea is protected underneath the upper eyelid with a brisk Bell’s phenomenon. Acute postoperative lateral skull base surgery patients with a complete facial paralysis may initially present with almost normal appearing eye closure, presumably owing to edema of the eyelids and orbicularis oculi muscle. However, lagophthalmos eventually develops after this immediate postoperative period. Corneal sensation should be assessed and compared with the unaffected side. Lacrimal secretion can be assessed using Schirmer’s test. Although eyelid approximation depends primarily on the movement of the upper eyelid, the position and slight movement of the lower eyelid is also important in ocular protection. Deviation of the lower eyelid from its normal position at the lower limbus owing to paralytic ectropion can impact the maintenance of an appropriate tear film causing dryness or epiphora, and even diminish the benefits of supplemental lubrication. In the setting of lower eyelid malposition, lower eyelid repositioning or tightening procedures should be considered to ensure adequate corneal protection. Lagophthalmos and ectropion secondary to facial paralysis cause poor tear film movement and tear evaporation, which can lead to exposure keratitis, corneal abrasion, and permanent vision changes, including blindness.
Indications for surgical intervention
The etiology and severity of the facial paralysis is an important factor in the management of the paralyzed eyelids. Upper eyelid loading procedures are usually indicated for patients with incomplete eye closure in whom spontaneous recovery is expected to be prolonged and/or incomplete. Additional indications include patients with a poor Bell’s phenomenon or sequelae of corneal exposure. Patients demonstrating rapid improvement of a facial paralysis may be considered for management with supplemental lubrication, moisture chambers, nighttime taping, and possibly a temporary tarsorrhaphy for a period of time to see if the eyelid function returns. Medical management for patients with upper eyelid paralysis should be reserved for patients with reliable access to regular ophthalmologic examinations, overall good health, and minimal other comorbidities. Upper eyelid loading procedures are the gold standard for surgical management of lagophthalmos in the setting of a paralyzed upper eyelid. These procedures are reversible and generally performed under local anesthesia.
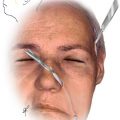
Preoperative testing in the office to determine the appropriate size weight is an important step in surgical planning ( Fig. 1 ). The test weight is centered over the medial limbus and is secured with double-sided adhesive to the upper eyelid. The weight is left attached for several minutes. The appropriate size weight allows effective eye closure without inducing ptosis. Eye closure should be assessed with the patient in the upright and supine positions to approximate the position of the weight and globe when the patient is awake and sleeping. Most patients require a 0.8, 1.0 or 1.2 g weight.