Orthopedic and orthodontic management of patients born with clefts of the lip, alveolus and palate is based on the application of basic biomechanical principles adapted to the individualized cleft anatomy. This article focuses on orthopedic and orthodontic preparation for 2 stages of interdisciplinary orthodontic/surgical cleft care: presurgical infant orthopedics (nasoalveolar molding) for lip/alveolus/nasal surgical repair and maxillary arch preparation for secondary alveolar bone grafting. These preparatory stages of orthopedic/orthodontic therapy are undertaken with the goal of restoring normal anatomic relationships to assist the surgeon in providing the best possible surgical care.
Key points
- •
The interdisciplinary approach to primary and secondary surgical procedures has been proven to be beneficial for patients.
- •
In the neonate, nasoalveolar molding has been found to optimize the aesthetic outcome of the nasal and labial repair while minimizing the extent of surgery and formation of scar tissue.
- •
During the mixed dentition stage, orthopedic arch preparation before the secondary alveolar bone-grafting procedure improves arch morphology, restores the functional interarch relationship, and facilitates surgical access.
- •
The cooperative effort between the surgeon and craniofacial orthodontist in designing strategies customized to the patient’s specific needs has resulted in better esthetic and functional outcomes, minimizing surgical interventions.
Introduction
An alveolar cleft refers to the space between the maxillary segments anterior to the incisive foramen, and therefore presents a discontinuity in the dental arch. Routine cleft lip repair and subsequent cleft palate repair do not specifically address the bony deficiency at this site. Consequently, strategies specifically designed to manage the alveolar cleft must be incorporated into the complete treatment itinerary, and require a cooperative effort of the craniofacial orthodontist and surgeon. Orthopedic and orthodontic management of patients born with clefts of the lip, alveolus, and palate is based on the application of basic biomechanical principles adapted to the individualized cleft anatomy. This article focuses on orthopedic and orthodontic preparation for 2 stages of interdisciplinary orthodontic/surgical cleft care: (1) presurgical infant orthopedics for primary lip/alveolus/nasal surgical repair; and (2) maxillary arch preparation for secondary alveolar bone grafting. These preparatory stages of orthopedic/orthodontic therapy are undertaken with the goal of restoring normal anatomic relationships to assist the surgeon in providing the best possible surgical care.
Introduction
An alveolar cleft refers to the space between the maxillary segments anterior to the incisive foramen, and therefore presents a discontinuity in the dental arch. Routine cleft lip repair and subsequent cleft palate repair do not specifically address the bony deficiency at this site. Consequently, strategies specifically designed to manage the alveolar cleft must be incorporated into the complete treatment itinerary, and require a cooperative effort of the craniofacial orthodontist and surgeon. Orthopedic and orthodontic management of patients born with clefts of the lip, alveolus, and palate is based on the application of basic biomechanical principles adapted to the individualized cleft anatomy. This article focuses on orthopedic and orthodontic preparation for 2 stages of interdisciplinary orthodontic/surgical cleft care: (1) presurgical infant orthopedics for primary lip/alveolus/nasal surgical repair; and (2) maxillary arch preparation for secondary alveolar bone grafting. These preparatory stages of orthopedic/orthodontic therapy are undertaken with the goal of restoring normal anatomic relationships to assist the surgeon in providing the best possible surgical care.
Presurgical infant orthopedics
The history of presurgical infant orthopedics (PSIO) dates back to 1686 when Hoffman described the use of an extraorally anchored headcap to place a retraction force on the premaxilla. A similar method is described in more contemporary literature, such as in Berkowitz’s 1996 article that described “a head bonnet with an external elastic that is sometimes used before surgical lip closure to ventroflex the premaxilla, thereby reducing tension at the surgical sites.” McNeil introduced intraorally anchored appliances in 1950, using a progressively modified feeding plate to align maxillary alveolar segments. Another popular variant of an intraoral device to mold the alveolar segments was introduced in 1980 by Latham ; this acrylic appliance was retained by pins to the alveolar segments and used a system of elastomeric material to move the alveolar segments in proximity. A more recent technique, nasoalveolar molding (NAM), was introduced in 1993 by Grayson and colleagues. This technique not only molds the cleft alveolus as in previous PSIO protocols but also shapes and forms the nasal cartilages in preparation for the primary surgical repair.
PSIO appliances have been described as either active or passive devices. Active appliances are fixed intraorally and apply traction through mechanical means such as elastic chains, screws, and plates (eg, the Latham appliance). A passive appliance maintains the distance between the 2 maxillary segments while external force is applied to the system. NAM is an example of a passive PSIO technique and is the focus of this article.
A recent study by Sischo and colleagues examined the prevalence of NAM among cleft centers in the United States. Among teams interviewed via telephone survey, 37% offered NAM therapy. It was speculated that the high prevalence of NAM therapy might be due to increased insurance coverage and growing adoption of this treatment approach.
Grayson and Santiago described the NAM protocol for cleft patients in 1997. NAM takes advantage of the high degree of plasticity of neonatal cartilages, molding the deformed cleft nose by incorporating a nasal stent to an alveolar molding plate. The overall goal of this presurgical orthopedic therapy is to restore the correct skeletal, cartilaginous, and soft-tissue anatomic relationships, providing the most optimal conditions for the primary lip, alveolus, and nose surgery. The intent is to create a lasting aesthetic outcome and reduce the need for, or minimize the extent of, secondary surgical revision procedures.
NAM objectives include:
- 1)
Molding and repositioning of the alveolar processes
- 2)
Molding and reposition of the nasal cartilages, and
- 3)
Lengthening of the deficient columella.
Short-term (4 months to 1 year) and long-term (4.5–9 years) studies indicate that NAM significantly improves nasal symmetry over surgery alone.
An adjunctive surgical option, gingivoperiosteoplasty (GPP) (closure of the soft-tissue alveolar segments), is possible if there is close approximation of the cleft alveolar segments. Santiago and colleagues have shown a 60% reduction in the need for a secondary alveolar bone-graft procedure in cases where a combined approach of PSIO and a GPP was performed. This combination was less expensive than a traditional protocol (lip repair, primary nasal repair, and secondary alveolar bone graft). It is important to note that GPP is a separate therapeutic option from NAM, associated with its own risks and benefits.
Timing of Cleft Surgical Preparation
Referral to the cleft team before birth is now commonplace if there is diagnosis of the cleft on ultrasonography. This timing affords an opportunity for the family to become acquainted with the concept of team care and learn the generalities of the treatment options. Early consultation with the treating surgeon and NAM provider to discuss the logistics of NAM therapy in preparation for the primary lip and nose surgical repair is an important first step toward the parents’ informed decisions regarding the collaborative care options.
Ideally, the interdisciplinary cleft team evaluates the neonate 1 week after birth. The cleft surgeon and craniofacial orthodontist perform a clinical examination, photos are taken, and an impression of the intraoral cleft defect is taken in a hospital setting with the surgeon as part of the impression team. This noninvasive procedure, during which the infant is fully awake and not anesthetized, is done using a premade acrylic impression tray and an elastomeric material ( Fig. 1 ).
The impression is then used to create a stone cast and a conventional acrylic molding plate. The molding plate is made of clear orthodontic resin, and 1 or 2 (depending of the deformity) buttons or extensions are added to the anterior part of the appliance. These buttons are made of stainless-steel orthodontic wire covered with clear resin material, and grooved to hold orthodontic elastics and surgical tapes used to control the force applied to the alveolar segments ( Fig. 2 ). The intraoral acrylic plate is examined for rough areas, polished, and inserted within a week of the initial visit. The molding plate is then modified on a weekly basis to approximate the intraoral segments and reduce the alveolar cleft. Once the segments are in close proximity, a nasal stent is added to mold the distorted nasal cartilages.
Correcting the unilateral deformity
The unilateral cleft lip and palate anomaly presents a significant nasal deformity; a detailed description of the cleft nasal deformity at infancy is provided in the article “Correction of the Cleft Nasal Deformity: From Infancy to Maturity” elsewhere in this issue by Marcus and colleagues. In brief, the lower lateral cartilage is depressed and concave on the cleft side and is separated from the contralateral cartilage located high in the nasal tip. This configuration results in depression and displacement of the nasal tip and lateralization of the nostril apex. The columella and nasal septum are inclined over the cleft with the base deviated toward the noncleft side ( Fig. 3 ).
The goals of NAM in patients with unilateral cleft lip and palate are to reduce the severity of the cleft deformity by approximating the alveolar and lip segments and correcting malposition of the nasal cartilages, nasal tip, philtrum, and columella. These corrections are achieved through periodic modifications of the intraoral molding plate and adjustments of the extraoral nasal stent.
At the NAM appliance insertion visit, the intraoral molding plate is seated, adjusted, and activated to provide alveolar movement. Intraorally the plate is activated by the selective addition and/or removal of hard and soft acrylic. Correction of the alveolar malposition and associated soft-tissue structures is achieved by weekly modifications of the molding plate, which allows for gradual and controlled approximation of the alveolar segments.
The extraoral activation system consists of 2 surgical tapes individually folded inside the lumen of 2 orthodontic elastics, which are placed on the channel of the acrylic button. The 2 strips are then stretched and taped over a wider facial tape used to protect the neonate from skin irritation, which helps to secure the molding plate to the palate and alveolar processes. Therefore, the tape and elastic construct is usually more active on the side toward the intended movement. As the effectiveness of the NAM therapy depends on the stability of the plate on the transported segment, some clinicians prefer to use a small amount of denture adhesive only on the segment to be mobilized ( Fig. 4 ).
Once the alveolar segments are in close approximation (around 4 mm), lip taping and a nasal stent are added to the system ( Fig. 5 ). Taping of the cleft lip segments in tight apposition assists the elastic orthopedic forces in achieving controlled approximation of the alveolar cleft segments. In addition, it improves alignment of the nasal base region by bringing the columella toward the midsagittal plane and improving symmetry of the nostril apertures. In select patients, lip taping can be started before the nasal stent is incorporated into the molding plate.
The nasal stent is constructed from an orthodontic wire carefully bent into a gooseneck shape, which is incorporated into the anterior flange of the oral molding plate. The most superior part of the wire is covered with hard and soft acrylic to ensure that tissue breakdown does not occur when positive pressure is applied to the nasal lining. The stent is positioned inside the nose underneath the apex of the alar cartilage on the cleft side. The alar dome cartilage on the cleft side is lifted by the stent to achieve normal elevation and symmetry.
The nasal stent is gradually modified on a weekly basis. The shape of the cartilaginous septum, dome, and medial and lateral crura are carefully molded to resemble the normal shape of these structures.
At the conclusion of nasal and alveolar molding, the nasal cartilages, columella, philtrum, and alveolar segments should be properly aligned to facilitate the surgical restoration of normal anatomic relationships ( Fig. 6 ).
Correcting the bilateral deformity
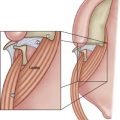
The bilateral deformity presents a different set of challenges. In the bilateral cleft, the alar cartilages have failed to migrate up into the nasal tip and elongate the columella. The alar cartilages are positioned along the alar margins and are stretched over the cleft as flaring alae. In addition, the premaxilla is suspended from the tip of the nasal septum, whereas the lateral alveolar segments remain behind. Disparate growth may occur, causing overprojection, flexion, or rotation of the premaxillary segment ( Fig. 7 ).
The goal of presurgical NAM in patients born with bilateral cleft lip and palate is to lengthen the columella, reposition the nasal cartilages toward the tip, and align the alveolar segments.
As in the unilateral deformity, an intraoral impression of the neonate is taken and a bilateral acrylic molding plate is fabricated. In contrast to the unilateral plate, the bilateral plate has 2 anterior wire and acrylic extensions or buttons. The first stage of treatment consists of retracting and uprighting the everted premaxilla into the space between the 2 lateral alveolar segments ( Fig. 8 ). This goal is achieved by weekly modifications of the intraoral molding plate and the use of orthodontic elastics and surgical tapes, as described for unilateral deformity. In the second stage of treatment, as the alveolar segments gradually approximate one another, 2 nasal stents are incorporated into the anterior rim of the molding plate and enter the nasal apertures ( Fig. 9 ). The nasal stents support the nasal tip and create tissue-expanding forces that are directed to the columella and domes internally. A surgical tape is applied to the prolabium, pulled down, and adhered to an orthodontic elastic attached to the 2 anterior buttons ( Fig. 10 ). A horizontal prolabial band made of soft acrylic may also be attached across the 2 nasal stents to depress the columella base in the region normally represented by the lip-columella junction, providing countertraction force to the columellar tissue. Each functional component of the bilateral system is gradually modified to mold the hard and soft tissues and achieve the desired goals ( Fig. 11 ).