Lymphatic malformation results from an error in the embryonic development of the lymphatic system. Clinically, lymphatic malformation is characterized by the size of the malformed channels: microcystic, macrocystic, or combined (microcystic/macrocystic).This article describes the clinical features, diagnosis, and management of lymphatic malformations.
Clinical features
Lymphatic malformation (LM) results from an error in the embryonic development of the lymphatic system. Sprouting lymphatics may become separated from the primitive lymph sacs or main lymphatic channels; alternatively, lymphatic tissue may form in an abnormal location. Clinically, LM is characterized by the size of the malformed channels: microcystic, macrocystic, or combined (microcystic/macrocystic). Macrocystic lesions are defined as cysts large enough to be treated by sclerotherapy. Because the lymphatic and venous systems share a common embryologic origin, phlebectasia can occur in association with LM. LM usually is noted at birth. A small or deep lesion, however, may not become evident until late childhood or adolescence when the lesion has grown large enough to cause a visible deformity or symptoms. LM is most commonly located on the head and neck; other frequent sites include the axilla, chest, and perineum. Lesions are soft and compressible. The overlying skin may be normal, have a bluish hue, or contain pink vesicles that can appear similar to a capillary malformation. Primary lymphedema is also a LM that usually presents in infancy or adolescence and most commonly involves the lower extremity. LM is particularly problematic because it is progressive; it slowly expands over time and recurs after treatment.
LM typically causes a deformity and psychosocial morbidity, especially when it involves the head and neck. The 2 most common complications are bleeding and infection. Bleeding results from abnormal venous channels in the malformation or from small arteries in the septi. Intralesional bleeding occurs in up to 35% of LMs causing bluish discoloration, pain, or swelling. LM is prone to infection because the malformed lymphatics are less able to clear foreign material and contribute to antibody production; proteinaceous fluid and blood in the cysts also favor bacterial growth. Infection complicates as many as 71% of lesions and can progress rapidly to sepsis. Poor dental hygiene predisposes to infection of cervicofacial malformations. Similarly, buttock or pelvic LM may be infected by translocation of gut flora. Cutaneous vesicles can bleed, cause malodorous drainage, and serve as a portal for bacteria. Osseous LMs can cause bony destruction. Swelling caused by bleeding, infection, or viral illness may obstruct vital structures.
Two-thirds of patients with cervicofacial LM require tracheostomy to maintain the airway. Secondary bony overgrowth is another complication; the mandible is most commonly involved, and patients can develop an open-bite and malocclusion. Jaw contouring or orthognathic procedures are required in three-fourths of patients with cervicofacial LM. Oral lesions can cause macroglossia, and vesicles are associated with bleeding, pain, poor oral hygiene, and caries. Thoracic or abdominal LM may lead to pleural, pericardial, or peritoneal chylous effusions. Intestinal LM can present as chronic malabsorption. Periorbital LM causes proptosis (45%), ptosis (52%), and amblyopia (33%); ultimately 40% of patients have a permanent reduction in vision and 7% become blind in the affected eye. Upper extremity LM can significantly limit function, and the brachial plexus may be involved if the lesion is located in the axilla. LM may be diffuse or multifocal (involving multiple noncontiguous areas); patients can have splenic involvement, chylous effusions, or osteolytic bone lesions.
Diagnosis
Ninety percent of LMs are diagnosed by history and physical examination. Small, superficial lesions do not require further diagnostic workup. However, large or deep LMs are evaluated by magnetic resonance imaging (MRI) to (1) confirm the diagnosis, (2) define the extent and type of malformation, and (3) plan treatment. MRI sequences are obtained with fat suppression, and gadolinium helps differentiate LM from venous malformation (VM). LM appears as a cystic lesion (macrocystic, microcystic, combined) with septations of variable thickness. Because LM has a high water content, it is hyperintense on T2-weighted sequences. After treatment, though, scar tissue causes LM to become less hyperintense. On T1-weighted images LM shows enhancement of the wall and septa unlike VM, which has heterogeneous patchy enhancement. Macrocystic lesions often have fluid levels because of intracystic blood or protein. Microcystic LM has more ill-defined borders and greater enhancement than macrocystic lesions. Unlike VM, LM is more likely to appear infiltrative.
Although ultrasonography (US) is not as informative as MRI, sedation in children is not required. US may provide diagnostic confirmation, document intralesional bleeding, and differentiate between macrocystic and microcystic lesions. US findings for macrocystic LM include anechoic cysts with internal septations, often with debris or fluid-fluid levels. Microcystic LM has ill-defined echogenic masses with diffuse involvement of adjacent tissues. Computed tomography and plain films are occasionally useful to delineate osseous involvement, particularly if resection is planned. Lymphedema can be diagnosed by lymphoscintigraphy.
Histologic confirmation of LM is rarely necessary because lesions are diagnosed by history, physical examination, and imaging. Histopathology is relatively nonspecific; LM shows abnormally walled vascular spaces with eosinophilic protein-rich fluid, and collections of lymphocytes. Immunostaining with the lymphatic markers D2-40 and LYVE-1 are positive. Biopsy may be indicated if imaging is equivocal or if a malignant process is suspected.
Diagnosis
Ninety percent of LMs are diagnosed by history and physical examination. Small, superficial lesions do not require further diagnostic workup. However, large or deep LMs are evaluated by magnetic resonance imaging (MRI) to (1) confirm the diagnosis, (2) define the extent and type of malformation, and (3) plan treatment. MRI sequences are obtained with fat suppression, and gadolinium helps differentiate LM from venous malformation (VM). LM appears as a cystic lesion (macrocystic, microcystic, combined) with septations of variable thickness. Because LM has a high water content, it is hyperintense on T2-weighted sequences. After treatment, though, scar tissue causes LM to become less hyperintense. On T1-weighted images LM shows enhancement of the wall and septa unlike VM, which has heterogeneous patchy enhancement. Macrocystic lesions often have fluid levels because of intracystic blood or protein. Microcystic LM has more ill-defined borders and greater enhancement than macrocystic lesions. Unlike VM, LM is more likely to appear infiltrative.
Although ultrasonography (US) is not as informative as MRI, sedation in children is not required. US may provide diagnostic confirmation, document intralesional bleeding, and differentiate between macrocystic and microcystic lesions. US findings for macrocystic LM include anechoic cysts with internal septations, often with debris or fluid-fluid levels. Microcystic LM has ill-defined echogenic masses with diffuse involvement of adjacent tissues. Computed tomography and plain films are occasionally useful to delineate osseous involvement, particularly if resection is planned. Lymphedema can be diagnosed by lymphoscintigraphy.
Histologic confirmation of LM is rarely necessary because lesions are diagnosed by history, physical examination, and imaging. Histopathology is relatively nonspecific; LM shows abnormally walled vascular spaces with eosinophilic protein-rich fluid, and collections of lymphocytes. Immunostaining with the lymphatic markers D2-40 and LYVE-1 are positive. Biopsy may be indicated if imaging is equivocal or if a malignant process is suspected.
Management
Nonoperative
LM is a benign condition, and intervention is not mandatory; small or asymptomatic lesions may be observed. Intralesional bleeding is treated conservatively with pain medication, rest, and occasionally prophylactic antibiotics because bleeding may predispose to infection. An infected LM often cannot be controlled with oral antibiotics, and intravenous antimicrobial therapy usually is required. Patients with more than 3 infections in 1 year are given daily prophylactic antibiotics. Because LM is at risk for infection, good oral hygiene should be maintained and patients should avoid incidental trauma. Lymphedema is managed by layered, custom-fitted compression garments as well as pneumatic compression.
Operative
Intervention for LM is reserved for symptomatic lesions that cause pain or significant deformity, or threaten vital structures. Most children do not require treatment at the time of diagnosis. Because LM slowly expands, however, patients may become symptomatic and seek intervention in childhood or adolescence. Less commonly, an LM involving an anatomically sensitive area or causing a deformity necessitates management as early as infancy. For example, a lesion obstructing the airway or visual axis requires urgent intervention. If possible, treatment may be postponed until after 12 months of age when the risk of anesthesia is lowest. Intervention for a lesion causing a visible deformity should be considered before 3.5 years to limit psychological morbidity; at this age long-term memory and self-esteem begin to form. Some parents, however, may elect to wait until the child is older and able to make the decision to proceed with operative intervention, especially if the deformity is minor.
Sclerotherapy
Sclerotherapy is first-line management for large or problematic macrocystic/combined LM. Sclerotherapy involves aspiration of the cysts followed by the injection of an inflammatory substance, which causes scarring of the cyst walls to each other. Although sclerotherapy does not remove the LM, it effectively shrinks the lesion ( Fig. 1 ). Sclerotherapy has superior efficacy and a lower complication rate than resection; it is 4 times more likely to be successful and has one-tenth the morbidity. Long-term control of LM also is favorable; more than 90% of patients treated with OK-432 do not have a regrowth of their lesion 3 years following treatment. Resection of macrocystic LM generally is not indicated unless (1) the lesion is symptomatic and sclerotherapy is no longer possible because all of the macrocysts have been treated, or (2) resection may be curative because the lesion is small and well localized.
Several sclerosants may be used to treat LM: doxycycline, sodium tetradecyl sulfate (STS), ethanol, bleomycin, and OK-432 (killed group Streptococcus pyogenes ). The authors prefer doxycycline because it is very effective (83% reduction in size) and safe. In addition, doxycycline theoretically may prevent infectious complications. Almost all macrocystic LMs have an excellent response; improvement for combined LMs is superior for lesions with a greater macrocystic composition. A solution of 10 mg/mL is injected, and up to 50 mL (500 mg) may be used for infants and small children; older children and adults may be treated with as much as 100 mL (1000 mg). STS is another effective agent; it probably has a higher complication rate than doxycycline. Bleomycin causes minimal swelling and is considered for lesions in difficult anatomic areas (eg, airway) or for LMs not responsive to other agents. Bleomycin may have some benefit for microcystic lesions that are not amenable to resection. Ethanol is an effective sclerosant but has the highest complication rate. It can be used for small lesions, but large volumes should be avoided to reduce the risk of local and systemic toxicity. Ethanol can injure nerves and, thus, should not be used in proximity to important structures (eg, facial nerve). However, with careful use and avoidance of extravasation, ethanol can be used safely for unresponsive lesions. OK-432 recently has been shown to be effective: 94% and 63% of patients with macrocystic or combined lesions, respectively, have greater than a 60% reduction in size with minimal morbidity. Patients with microcystic LM do not respond to OK-432. OK-432, however, is not widely available.
Small lesions, particularly in adolescents and adults, may be treated in the office without image guidance; 3% STS is diluted with saline to inject a 1% solution. Most patients, especially children, are managed under general anesthesia. Lesions are treated using US with or without fluoroscopy. Contrast can be injected to determine the anatomy of complex lesions, but contrast injection is not usually required. The volume of contrast used to opacify the lesion is less than the amount of sclerosant that is subsequently delivered. After aspirating fluid from the cyst, the sclerosant is injected. Large cysts occasionally require pigtail catheter placement and sequential drainage and injection over several days. Resolution of macrocysts may occur within days, but may take up to 6 to 8 weeks. Depending on the size of the malformation, and whether there is a residual macrocystic component, additional injections every 6 to 8 weeks may be necessary.
Posttreatment edema progresses for 24 to 48 hours after the procedure. Except for young infants and airway lesions, most patients are discharged home the same day. Dexamethasone is not administered routinely. Posttreatment edema, especially around the airway, may necessitate close monitoring in the intensive care unit; occasionally prolonged intubation or tracheostomy is required. Orbital injections, even with minor extravasation, can cause orbital compartment syndrome, and patients are examined postoperatively by an ophthalmologist. Because LM is at risk for infection, patients are given perioperative antibiotics.
The most common complication of sclerotherapy is skin ulceration (<5%), which is more likely with superficial lesions and when ethanol is used. Ulceration is managed with local wound care; the wound is allowed to heal secondarily. STS and doxycycline are not associated with significant systemic adverse effects. In contrast, ethanol can cause central nervous system depression, pulmonary hypertension, hemolysis, thromboembolism, and arrhythmias. Transient (5%) or permanent (2.5%) nerve injury is rare after ethanol sclerotherapy, and has not been noted to occur with doxycycline or STS. LM may reexpand over time; 9% recur within 3 years after OK-432 treatment and most enlarge with longer follow-up. Consequently, patients often need repeat sclerotherapy over the course of their lifetime. If a problematic LM recurs and macrocysts are no longer present, then resection is the next treatment option.
Resection
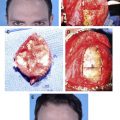
Extirpation of LM can be associated with significant morbidity: major blood loss, iatrogenic injury, and deformity. For example, resection of cervicofacial LM can injure the facial nerve (76%) or hypoglossal nerve (24%). Excision is usually subtotal because LM involves multiple tissue planes and important structures; recurrence is common (35%–64%). Even after complete extirpation, at least 17% of lesions reexpand. Consequently, sclerotherapy is the preferred treatment for macrocystic/combined lesions. Nonproblematic microcystic lesions can be observed. Resection is reserved for (1) small, well-localized LM (microcystic or macrocystic) that may be completely excised for cure ( Fig. 2 ), (2) symptomatic microcystic LM ( Fig. 3 ), and (3) symptomatic macrocystic/combined LM that no longer can be managed with sclerotherapy because all macrocysts have been treated. When considering resection, the postoperative scar/deformity after removal of the LM should be weighed against the preoperative appearance of the lesion.
Related posts:
 Vascular Anomalies: Current Overview of the Field
Vascular Anomalies: Current Overview of the Field
 Pathogenesis of Vascular Anomalies
Management of Venous Malformations
Pathogenesis of Vascular Anomalies
Management of Venous Malformations
 Management of Arteriovenous Malformations
Management of Arteriovenous Malformations
 Management of Combined Vascular Malformations
Management of Combined Vascular Malformations
 Special Considerations in Vascular Anomalies: Operative Management of Craniofacial Osseous Lesions
Special Considerations in Vascular Anomalies: Operative Management of Craniofacial Osseous Lesions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


