Vascular tumors of childhood are typically benign. The 4 most common types are infantile hemangioma (IH), congenital hemangioma (CH), kaposiform hemangioendothelioma (KHE), and pyogenic granuloma (PG). Vascular tumors must be differentiated from vascular malformations. Although tumors and malformations may appear as raised, blue, red, or purple lesions, their management differs significantly.
Vascular tumors of childhood are typically benign. The 4 most common types are infantile hemangioma (IH), congenital hemangioma (CH), kaposiform hemangioendothelioma (KHE), and pyogenic granuloma (PG). Vascular tumors must be differentiated from vascular malformations. Although tumors and malformations may appear as raised, blue, red, or purple lesions, their management differs significantly.
Infantile hemangioma
Clinical Features
IH is a benign tumor of the endothelium, and the most common tumor of infancy. IH affects approximately 4% to 5% of Caucasian infants and is rare in dark-skinned individuals. It is more frequent in premature children (23% of infants <1200 g) and females (3:1 to 5:1). IH typically is single (80%) and involves the head and neck (60%), trunk (25%), or extremity (15%). The median age of appearance is 2 weeks, although 30% to 50% of lesions are noted at birth as a telangiectatic stain or ecchymotic area. IH grows faster than the rate of the child during the first 9 months of age (proliferating phase); 80% of its size is achieved by 3.2 (±1.7) months. When IH involves the superficial dermis it appears red. A lesion beneath the skin may not be appreciated until 3 to 4 months of age when it has grown large enough to cause a visible deformity; the overlying skin may appear bluish. By 9 to 12 months of age the growth of IH plateaus to approximate that of the infant. After 12 months of age the tumor begins to shrink (involuting phase); the color fades and the lesion flattens ( Fig. 1 ). Involution stops in most children by 5 years of age (involuted phase). After involution, one-half of children have an abnormality: residual telangiectasias, anetoderma from loss of elastic fibers, scarring, fibrofatty residuum, redundant skin, or destroyed anatomic structures.

Diagnosis
Ninety percent of IH are diagnosed by history and physical examination ( Fig. 2 ). Deeper lesions may be more difficult to appreciate because they are noted later than superficial tumors, and may not have significant overlying skin changes. Diagnosis of subcutaneous IH is facilitated using a hand-held Doppler device showing fast flow. When history and physical examination are equivocal, ultrasonography is the first-line confirmatory study to differentiate IH from other lesions. IH appears as a soft-tissue mass with fast flow, decreased arterial resistance, and increased venous drainage. Magnetic resonance imaging (MRI) can differentiate vascular anomalies, although young children require sedation. During the proliferating phase, IH is isointense on T1 images, hyperintense on T2 sequences, and enhances with contrast. IH appears as a mass with dilated feeding and draining vessels; signal voids represent fast flow and shunting. Involuting IH has increased lobularity and adipose tissue; the number of vessels and flow is reduced.

Rarely, biopsy is indicated if malignancy is suspected or if the diagnosis remains unclear following imaging studies. Tumors or fast-flow lesions that may be confused with IH include arteriovenous malformation, CHs, cutaneous leukemia (chloroma), hemangioendotheliomas, infantile fibrosarcoma, infantile myofibromatosis, lymphoma, metastatic neuroblastoma, PTEN-associated vascular anomaly, and PG. In the liver, the differential diagnosis of hemangioma includes arteriovenous malformation, hepatoblastoma, or metastatic neuroblastoma. Because an erythrocyte-type glucose transporter (GLUT1) is specifically expressed in IH, immunostaining for GLUT1 can differentiate IH from other tumors and malformations.
Clinical Considerations
Head and neck hemangiomas
Ten percent of proliferating IH cause significant deformity or complications, usually when located on the head or neck. Ulcerated lesions may destroy the eyelid, ear, nose, or lip. IH of the scalp or eyebrow can injure hair follicles, resulting in alopecia. Obstruction of the external auditory canal can cause otitis externa, but sensorineural hearing loss does not occur if the contralateral canal is patent. Periorbital hemangioma can block the visual axis or distort the cornea causing deprivation or astigmatic amblyopia, respectively. IH involving the upper eyelid is more likely to be problematic than a lesion involving the lower eyelid. Infants with periorbital IH are referred to an ophthalmologist; the noninvolved eye may be patched for a minimum of 2 hours per day to stimulate use of the affected eye. Subglottic hemangioma, associated with large cervicofacial lesions, may obstruct the airway; patients are referred to an otolaryngologist for evaluation. Although the patency of the airway is usually maintained with oral corticosteroid, laser treatment or tracheostomy may be necessary.
Multiple hemangiomas
Although 20% of infants have more than one IH, occasionally a child will have 5 or more small (<5 mm), dome-like lesions termed disseminated hemangiomatosis. These children are at increased risk for IH of internal organs, although the risk is low. The liver is most commonly affected; the brain, gut, or lung are rarely involved. Ultrasonography should be considered to rule out hepatic IH. However, because intervention is not necessary for an incidentally found liver lesion, families may not elect to pursue imaging. In addition, infants with problematic hepatic IH are usually symptomatic early in infancy, before they are referred for evaluation of the cutaneous lesions. If symptomatic brain, gut, or lung lesions are suspected, MRI is considered.
Hepatic hemangiomas
The liver is the most common extracutaneous site for IH, which may be focal, multifocal, or diffuse. Although hepatic IH usually are nonproblematic and discovered incidentally, large tumors can cause heart failure, hepatomegaly, anemia, or hypothyroidism. Ninety percent of fast-flow hepatic lesions are hemangioma; arteriovenous malformation, hepatoblastoma, and metastatic neuroblastoma are less common and do not demonstrate significant shunting on imaging. Focal hepatic IH usually is asymptomatic and not associated with cutaneous lesions; it is discovered incidentally on prenatal or antenatal ultrasonography. A focal liver hemangioma may not be IH but rather rapidly involuting congenital hemangioma (RICH), because it undergoes rapid postnatal involution and does not stain for GLUT1. Multifocal hepatic IH may be associated with cutaneous lesions and is immunopositive for GLUT1. Although usually asymptomatic, multifocal lesions can cause high-output cardiac failure because of shunting which is managed by corticosteroids with or without embolization. Diffuse hepatic IH can cause massive hepatomegaly, respiratory compromise, or abdominal compartment syndrome. Infants also are at risk for hypothyroidism and irreversible brain injury because the tumor expresses a deiodinase that inactivates thyroid hormone. Patients require thyroid-stimulating hormone monitoring and, if abnormal, intravenous thyroid replacement until the IH has involuted.
Reticular hemangioma
Reticular hemangioma is an uncommon variant of IH that most commonly affects the lower extremity and perineum; the involved limb is often undergrown. The macular lesion stains for GLUT1 and females (83%) usually are affected. Unlike typical IH, reticular tumors are: (1) infiltrative and not lobular; (2) involve fascia, muscle, or bone; and (3) are more likely to ulcerate and cause cardiac overload. Reticular hemangioma also may be associated with hepatic hemangioma as well as ventral-caudal anomalies (omphalocele, rectovaginal fistula, vaginal/uterine duplication, solitary/duplex kidney, imperforate anus, tethered cord). After involution small veins often remain, which may be treated by sclerotherapy.
Lumbosacral hemangioma
Large, superficial, plaque-like, or reticular IH rarely may be associated with underlying spinal, urogenital, or anorectal malformations when it is located in the lumbosacral midline (tethered cord, imperforate anus, abnormal genitalia, renal anomalies, lipomyelomeningocele). Ultrasonography is obtained to rule out associated anomalies in infants younger than 4 months. MRI is indicated in older infants or when ultrasonography is equivocal.
PHACE association
PHACE association affects 2.3% of all patients with IH, and consists of a plaque-like IH in a “segmental” or trigeminal dermatomal distribution of the face with at least one of the following anomalies: P osterior fossa brain malformation, H emangioma, A rterial cerebrovascular anomalies, C oarctation of the aorta and cardiac defects, E ye/ E ndocrine abnormalities. When ventral developmental defects ( S ternal clefting or S upraumbilical raphe) are present the condition is termed PHACES association. Ninety percent of infants are female and cerebrovascular anomalies are the most common associated finding (72%). Less than one-third of children have more than one extracutaneous feature. Because 8% of children with PHACE have a stroke in infancy and 42% have a structural brain anomaly, patients with suspected PHACE association should have an MRI to evaluate the brain and cerebrovasculature. If an anomaly is present, neurologic consultation is obtained. Aspirin therapy may be considered to reduce the risk of stroke if a cerebrovascular malformation is noted. Patients also should be referred for ophthalmologic, endocrine, and cardiac evaluation to rule out associated anomalies.
Nonoperative Management
Observation
Most IH are managed by observation because 90% are small, localized, and do not involve aesthetically or functionally important areas ( Fig. 3 ). Infants are followed closely, on a monthly basis, during the proliferative phase if a lesion has the potential to cause obstruction, destruction, or ulceration requiring intervention. Once the IH has stabilized in growth, patients are followed annually during the involuting phase if intervention may be necessary in childhood for excess skin, residual fibrofatty tissue, or to reconstruct damaged structures.

Wound care
During the proliferative phase at least 16% of hemangiomas ulcerate at a median age of 4 months; labial, neck, and anogenital tumors are most likely to ulcerate. Superficial IH is prone to skin breakdown because the integument is damaged by the tumor. In addition, arteriovenous shunting reduces capillary oxygen delivery and thus the skin is ischemic. Consequently, desiccation or minor injury can cause a wound to form; tumors located in trauma-prone areas are most likely to ulcerate. To reduce the risk of ulceration, the IH is kept moist during the proliferative phase with hydrated petroleum to minimize desiccation as well as to protect against accidental shearing of the skin. IH in the anogenital area may be further protected by using a petroleum gauze barrier to prevent friction from the diaper.
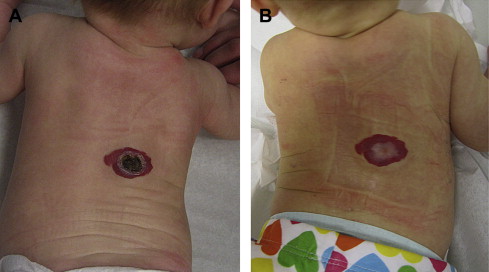
If ulceration develops, the wound is washed gently with soap and water at least twice daily. Small, superficial areas are managed by topical antibiotic ointment and occasionally with a petroleum gauze barrier ( Fig. 4 ). Large, deep wounds require damp-to-dry dressing changes. To minimize discomfort, a small amount of topical lidocaine may be applied no more than 4 times daily to avoid toxicity. EMLA (eutectic mixture of local anesthetics) contains prilocaine and should not be used in infants younger than 3 months because of the risk of methemoglobinemia.
Related posts:
 Vascular Anomalies: Current Overview of the Field
Vascular Anomalies: Current Overview of the Field
 Pathogenesis of Vascular Anomalies
Management of Venous Malformations
Pathogenesis of Vascular Anomalies
Management of Venous Malformations
 Management of Arteriovenous Malformations
Management of Arteriovenous Malformations
 Management of Combined Vascular Malformations
Management of Combined Vascular Malformations
 Special Considerations in Vascular Anomalies: Operative Management of Craniofacial Osseous Lesions
Special Considerations in Vascular Anomalies: Operative Management of Craniofacial Osseous Lesions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


