Gustilo IIIC injuries of the lower extremity pose a significant challenge to the reconstructive surgeon. Key principles include early vascular repair and serial debridement followed by definitive coverage within 10 days. Primary reconstructive options following vascular repair include the anterolateral thigh flap or the latissimus dorsi muscle flap. Complications include elevated rates of microvascular thrombosis requiring return to the operating room, partial and complete flap loss, and infection. There is also an elevated rate of secondary amputation. However, in spite of higher complication rates, when approached thoughtfully and with an experienced multidisciplinary team, patients can achieve reasonable functional outcomes.
Key points
- •
Gustilo IIIC injuries of the lower extremity are characterized by open tibia fractures with associated vascular injury requiring repair.
- •
These injuries pose a challenge to the reconstructive surgeon, and controversy remains regarding limb salvage versus primary amputation in these patients.
- •
Early recognition of vascular injury and subsequent repair is critical, in addition to early and serial debridement with the goal of achieving definitive reconstruction within 7 to 10 days after the injury.
- •
Reconstructive options for these injuries frequently require free tissue transfer, with the anterolateral thigh flap and the latissimus dorsi myofascial or myocutaneous flaps as the most common flaps used.
Introduction
Lower extremity fractures are a commonly encountered injury with epidemiologic surveys estimating rates of approximately 17 per 100,000 person years. These fractures occur along a spectrum of severity, with open fractures representing 2.6% of injuries. Most of these open fractures occur in young men as the result of high-energy trauma; however, elderly women involved in lower energy mechanisms also represent a significant proportion of these injuries. Open fractures are classified based on the Gustilo-Anderson Classification, with Gustilo IIIC injuries defined as open fractures with associated arterial injury requiring repair.
Fortunately, Gustilo IIIC injuries are relatively uncommon. Among studies specifically evaluating open tibial fractures, rates of IIIC injuries range from 2.5% to 3.4%. , Historically, these injuries have the worst prognosis of those patients requiring limb salvage with amputation rates ranging from 20% to as high as 75% to 77% in some studies. , Numerous investigators have devised a variety of scales and scoring criteria in an attempt to better determine which limbs should proceed to salvage versus primary amputation; however, there is no consensus on their reliability, and they have not been found to be predictive of functional recovery. As a result, the management of these injuries remains controversial.
Proponents of primary amputation cite increased length of stay, increased number and complexity of surgical procedures, high complication rates, and increased cost as the rationale favoring amputation. However, a systematic review of the existing literature on this topic that evaluated complications following limb salvage and amputation in type IIIB and IIIC injuries including osteomyelitis, nonunion, secondary amputation, ischemia, and flap failure did not find significant differences in duration of hospitalization, pain, limb function, or long-term quality of life between the groups.
Equivalent functional outcomes have also been observed when evaluating those patients undergoing reconstruction versus those patients undergoing amputation. In addition, when specifically evaluating cost, several studies have evaluated long-term costs between limb salvage and amputation and have found that patients undergoing amputation incur substantially higher lifetime costs compared with those patients treated with limb salvage.
Lastly, over the course of the nearly 40 years since Gustilo’s landmark publication on the topic, significant advancements in initial trauma management, vascular reconstruction, orthopedic fixation, and microvascular techniques have resulted in improved outcomes in this patient population. Single institution data demonstrate a statistically significant decrease in flap failure rates when patients are stratified by timing of reconstruction within their cohort. However, complication rates remain high in these patients due to the significant degree of trauma, with recent studies citing a 9% partial and 15.6% complete flap loss rate, so it is essential to approach these complex patients thoughtfully and in the context of an experienced, multidisciplinary team.
Reconstructive philosophy
Various reconstructive options exist for the management of Gustilo IIIC injuries, and determination of the optimal technique is individualized based on the following :
- •
Mechanism of injury
- •
Location and severity of the injury
- •
Degree of soft tissue deficit
- •
Other concomitant injuries
- •
Comorbidities
The goals of reconstruction include the following:
- •
Restoring form and function
- •
Promoting bony union
- •
Restoring sensation
- •
Minimizing donor site morbidity
Initial evaluation
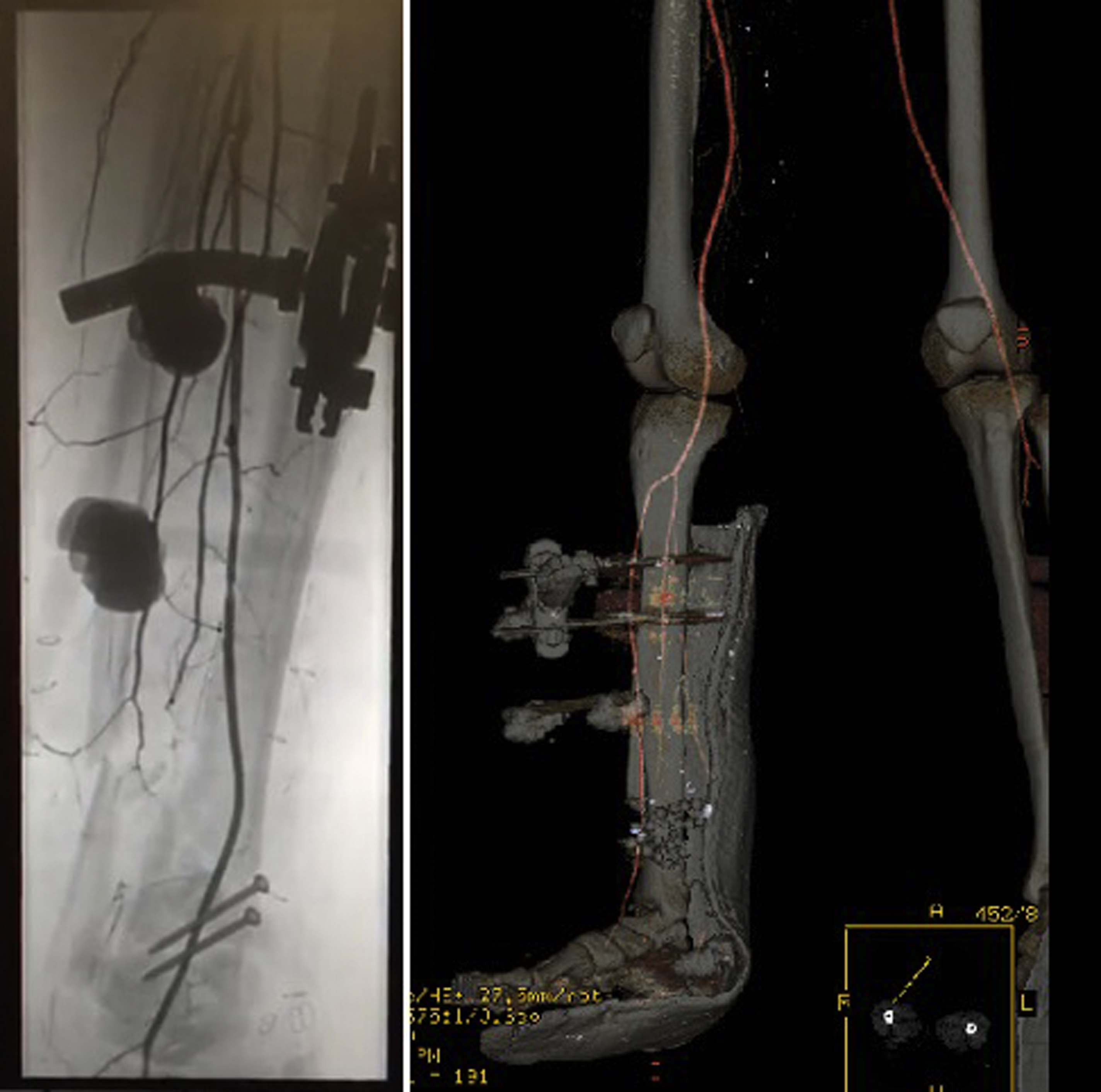
Gustilo IIIC injuries are often the result of high-energy trauma, so the initial evaluation based on advanced trauma life support (ATLS) is essential to ensure patient stability and address any immediately life-threatening injuries. Once the patient is deemed adequately stable, clinical examination of the affected limb including documentation of the pulse examination is crucial. Fig. 1 demonstrates those findings seen in a typical Gustilo IIIC injury with significant bony, soft tissue, and vascular injury.

Some debate in the literature exist as to the role of computed tomography (CT) angiograms in this patient population, but many investigators advocate for inclusion of this study in the evaluation if any of the following are present :
- •
Abnormal pulse or Doppler examination
- •
Zone of injury over potential free flap recipient vessels
- •
Zone of injury over any portion of a candidate regional flap and its blood supply
- •
Extensive soft-tissue or bony destruction from high-energy mechanism
- •
Preexisting arterial occlusive disease
In addition, CT angiography represents a less expensive and less invasive option than formal angiography. However, intraoperative angiography remains the gold standard for evaluation of these injuries, and an obviously dysvascular limb should be taken to the operating room emergently following initial ATLS stabilization barring any additional life-threatening injuries requiring intervention.
Antibiotics are another important component in the early management of these patients. Time to receipt of antibiotics after open fracture has been demonstrated to decrease rates of infection, specifically if received within 66 minutes of the injury. Typical regimens include a first-generation cephalosporin, such as cefazolin, as well as gentamycin.
Other immediate interventions that should be initiated in these patients include administration of a tetanus vaccine. , Many investigators also advocate for administration of low-molecular-weight heparin.
Timing of operative interventions
Generally, these patients are taken to the operating room within hours of presentation for evaluation, vascular repair, debridement, fasciotomies, and skeletal stabilization. At the time of this initial surgical intervention, the plastic surgeon can provide valuable insight, including the following , :
- •
Debridement of devitalized tissues and management of marginal skin flaps
- •
Incision planning to preserve regional flap options
- •
Optimal placement of external hardware to allow easier access to potential recipient vessels
We may also be able to aid in the critical determination as to whether primary amputation is indicated. Although decreasing in frequency, the primary amputation rate remains around 17%. Clinical situations that may merit primary amputation include the following , :
- •
Warm ischemia time exceeding 4 to 6 hours
- •
Muscle loss affecting more than 2 lower extremity compartments
- •
Bone loss exceeding more than one-third the length of the tibia
- •
Those patients deemed not reconstructable by the multidisciplinary surgical team
The timing of definitive reconstruction depends on the severity of the injury, need for serial debridement, and the patient’s other medical needs. Most of the publications evaluating time to coverage outcomes have evaluated IIIa and IIIb injuries, and the application of these results to the more severe IIIC injuries should be considered in the context of each clinical presentation. Some investigators advocate for the “fix and flap” principle with radical debridement, skeletal stabilization, neurovascular repair, and immediate soft tissue reconstruction. , However, several studies have demonstrated equivalent outcomes when definitive soft tissue coverage is performed within 3 days of injury. , When it is not possible to complete the reconstruction within 3 days, there is an increase in overall complications; however, recent evidence demonstrates no differences in flap outcomes, including flap failure and major complications, if performed by 10 days. With these data in mind, one should aim to achieve soft tissue reconstruction by 10 days postinjury whenever feasible.
Flap selection
Because of the extent of soft tissue and vascular injury, most of these fractures require free tissue transfer with a limited, supplemental role for local flaps. For IIIC injuries, most of the publications to date favor muscle over fasciocutaneous flaps. One study evaluated their flap choices and found that 40% were latissimus muscle flaps and 27% were anterolateral thigh flaps (ALT). This preferential use of the latissimus dorsi muscle flap seems to be true for multiple investigators, with others citing a 75% rate of muscle flaps with the latissimus dorsi used in 53% of those cases and was the most commonly used flap overall. Interestingly, studies evaluating the performance of muscle flaps versus fasciocutaneous flaps have found comparable rates of limb salvage and functional recovery between the 2 flap types. We have also found fasciocutaneous flaps easier to elevate for subsequent orthopedic revisions and therefore recommend assessing this factor based on the underlying bone quality and fixation method used at the time of flap coverage. Muscular segments either in combination with a fasciocutaneous flap, as the vastus lateralis with the ALT, or primary muscle flaps can be useful for filling in the more complex 3-dimensional bone loss defects, especially if not being filled in a Masquelet fashion with antibiotic cement.
An additional consideration should include flap size, as increased flap size has been correlated with increased rates of major complications including partial and complete flap loss. Specifically, for flaps greater than 250 cm 2 the rate of major complications is 50% versus 33.6% in less than 250 cm 2 flaps, and the rate of flap failure is 25% versus 11.8%. Increased flap size is an independent predictor of these outcomes, particularly in muscle flaps. Although these findings may be related to flap size serving as a surrogate marker for overall injury severity, they nevertheless provide another variable associated with lower extremity trauma-free flap outcomes. Similar to the timing data reviewed earlier, however, most of the literature is derived from IIIB free flap outcomes and extrapolated to these IIIC injuries.
Primary factors influencing free flap selection:
- •
Location and size of the defect
- •
Missing components (skin, muscle, nerve, bone), specifically what needs free tissue coverage and what can be skin grafted
- •
Vascular bypass conduit type, inflow, and outflow
- •
Length of vascular pedicle required to perform anastomosis outside of the zone of injury
- •
Potential recipient vessels (keep in mind that arterial inflow and venous outflow may not be possible in same recipient location)
- •
Vein graft source for grafting or arteriovenous loop
- •
Minimizing donor site morbidity
Surgical approach
A full understanding of the residual and novel revascularized anatomy is paramount to approaching these complex reconstructions, starting with being available for consultation during the emergent stabilization and revascularization to assist in initial management decisions. A multidisciplinary approach with early and active plastic surgery involvement preserves any residual soft tissue options, optimizes wound management, and provides a more complete evaluation of the defect. Other key steps include the following:
- •
Serial debridements, including soft tissue and bone, every 48 to 72 hours are often required before definitive coverage and should be part of the reconstructive plan.
- •
Study the angiogram and plan for multiple recipient vessel options but expect to use vein grafts and determine potential sources preoperatively.
- •
Have orthopedic surgery available to adjust fixation as needed, to make your dissection approach more straightforward.
- •
Primary shortening of the limb with a bone gap is an option, if needed.
- •
Set up the bone for primary repair with immediate coverage or delayed repair after a planned period of healing.
Ideally, a flap is selected that provides adequate soft tissue coverage with ample pedicle length for arterial and venous anastomoses performed beyond the zone of injury in close proximity to each other. In our experience, however, that is unfortunately the exception in these cases and there should be a low threshold to use vein grafts or an arteriovenous loop to complete the microvascular anastomosis. If vein grafting is required, every attempt should be made to reach source vessels as far out of the zone of injury as possible.
When feasible, our prefer to use either the disrupted anterior tibial or posterior tibial vessels proximal to the zone of injury away from the bypass graft and perform end-to-end anastomoses because the distal flow has been disrupted by the injury. Evaluation of our experience, however, has demonstrated higher flap complication rates using injured recipient vessels. We interpret this finding to highlight the insidious nature of the zone of injury—meticulous recipient vessel dissection and inspection are of utmost importance. Although recipient vessels proximal to the zone of injury are typically preferred, our experience does support distal anastomoses from retrograde flow off of the vascular bypass as a viable option without any evidence of increased flap loss. When feasible, the authors’ preference is to perform 2 venous anastomoses.
Postoperative care and expected outcome
Despite the often higher level of injury in these patients with IIIC injuries, once free flap coverage has been performed they usually follow standard lower extremity free flap protocols. However, significant heterogeneity exists in the postoperative management of these patients and seems to be largely dictated by surgeon preference.
Flap monitoring protocols typically involve frequent nursing and physician examination including use of a hand-held doppler probe, with some centers also using objective devices such as implantable dopplers or near infrared spectroscopy devices that monitor changes in tissue oxygenation. Regardless of the protocol used, for lower extremity flaps specifically, the data suggest that routine monitoring should be continued for at least 4 days as take-backs occur at an average of 3.7 days postoperatively. We have found suspending limbs from a trapeze via their external fixator frame or a calcaneal pin placed after the free flap to be extremely helpful in maintaining flap elevation during this early period, especially in this cohort with higher complication rates.
Although the evidence suggests equivalent functional recovery and flap failures between muscle flaps and fasciocutaneous flaps, it is important to recognize that fasciocutaneous flaps do have a more frequent take-back rate for suspected vascular compromise. Fortunately, fasciocutaneous flaps have a higher successful salvage rate as compared with muscle flaps, which is posited to be the result of lower metabolic demand in fasciocutaneous flaps and more easily recognized vascular compromise. It is important to keep these factors in mind when monitoring these flaps postoperatively to maximize the potential for early recognition and flap salvage.
The decision regarding the initiation of flap dependency training is also surgeon and institution dependent, with little high-level evidence to support a specific protocol. Most of the centers begin flap training in the 3 to 7 postoperative day range, and the available data do not show any increased rates of flap compromise with earlier, more aggressive protocols. We typically initiate flap dependency training around the seventh postoperative day but adjust accordingly depending on the stability of the flap, difficulty of the case, episodes of vascular compromise either during the index procedure or postoperatively, and the overall appearance of the flap including persistence of postoperative edema. Weight-bearing status is typically a joint decision with the orthopedic surgeon managing the patient’s bony injury.
Antibiotic duration is also quite variable and controversial, as infection remains one of the most significant complications after open fracture. Recent attempts at systematic review reveal a lack of robust literature on the subject and as a result they concluded that antibiotic prophylaxis is indicated in the immediate management of open tibia fractures but that the ideal duration remains unanswered.
Discharge disposition of these patients is often dictated by their other medical needs and traumatic injuries; however, the majority are able to discharge home after their hospitalization. Regardless of the patient’s disposition, specific attention should be paid to the postoperative rehabilitation protocol, as these injuries have the potential to substantially impact functional status and the ability to live independently. Despite the severity of these injuries, recent studies have documented an 83% limb salvage rate in this population. ,
Management of complications
Despite appropriate management, patients with IIIC injuries continue to experience substantial major complications including the following:
- •
Infection
- •
Thrombosis of arterial reconstruction resulting in limb ischemia
- •
Partial flap loss
- •
Complete flap loss
- •
Nonunion
- •
Secondary amputation
Infection rates for these injuries are approximately 35% and are best managed when diagnosed early and treated with prompt antibiotic therapy and serial debridements, followed by appropriate wound closure. , Infection can also include hardware and poorly vascularized retained bony segments, which should be thoughtfully dealt with in combination with your orthopedic colleagues.
Partial and complete flap loss rates have improved; however, they remain substantial in this population with some investigators reporting double the rates of microvascular thrombosis in patients with IIIC injuries as compared with other less severe injury patterns. Recent data found that only 75% of patients underwent reconstruction without flap loss, with a 9.4% partial flap loss rate and 15.6% complete flap loss rate. Other studies corroborate these findings, reporting flap loss rates ranging from 15% to 27%. ,
Rates of secondary amputation are variable and have improved over time, decreasing from 42% in early studies to as low as 5.5% more recently, although typical rates seem to range from 16% to 20%. , Causes of secondary amputation include infection, ischemia, and flap loss resulting in inability to achieve soft tissue coverage. The presence of arterial injury seems to be associated with these elevated amputation rates, with one study reporting a rate of 11.5% in patients with arterial injury compared with 1.5% in those without arterial injury.
Revision or subsequent procedures
Secondary revision procedures are common in this patient cohort, with some studies reporting a mean of 2.9 procedures performed. This reinforces the benefit of easier reelevation of fasciocutaneous flaps compared with muscle and should be considered during flap selection. Common secondary procedures include the following :
- •
Bone grafting
- •
Tendon reconstruction
- •
Flap debulking
- •
Flap liposuction
- •
Scar revision
Case demonstrations
Case 1
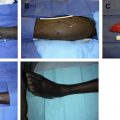
A 33-year-old man sustained a right lower extremity Gustilo IIIC injury following a motorcycle crash. He initially underwent revascularization of his anterior tibial artery using a reverse saphenous vein graft ( Fig. 2 ). He was also noted to have transection of his tibial nerve with a 10 cm gap, comminuted distal tibial and fibular shaft fractures, disruption of the Achilles tendon, and 30 cm by 15 cm soft tissue defect ( Fig. 3 ). After 2 debridements, in a joint procedure with orthopedic surgery he underwent open reduction and internal fixation of the right tibia, tibial nerve reconstruction with sural nerve cable grafting, Achilles tendon reconstruction with vascularized tensor fascia lata and iliotibial band, and soft tissue coverage with a left anterolateral thigh flap and split-thickness skin grafts ( Fig. 4 ). The anterolateral thigh flap was anastomosed end to end to the disrupted posterior tibial artery, and 2 venous anastomoses were performed using 3.0 and 2.0 venous couplers, respectively. The left thigh donor site and the lateral foot were then skin grafted to complete the reconstruction.
Related posts:
 Propeller Flaps in Lower Extremity Reconstruction
Propeller Flaps in Lower Extremity Reconstruction
 The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
 Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
 Orthoplastic Approach to Lower Extremity Reconstruction
Orthoplastic Approach to Lower Extremity Reconstruction
 The Anterolateral Thigh Perforator Flap
The Anterolateral Thigh Perforator Flap
 Lower Extremity Reconstruction in the Pediatric Population
Lower Extremity Reconstruction in the Pediatric Population
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


