Abstract
A thorough knowledge of the anatomy of the forehead and scalp is essential. Movement of muscles on the forehead are relayed through the brain and redirected to affect the innervation of the full forehead and scalp. This knowledge is used to develop the art of predicting expected results when any single muscle is paralysed with botulinum toxin. The author uses botulinum toxin on the forehead to block contraction of a muscle, or to increase the signalling to the contralateral muscle. The scalp movement must always be examined and predicted before modifying the action of a forehead muscle. The resting tone of the forehead and soft tissues must be noted, in particular, the height of the upper lids. If the lids ‘droop’ (ptosis), ptosis should be corrected surgically prior to management of rhytids. Severe dermatochalasis should also be treated surgically or the patient will be unhappy with the unfolding of heavy bags over their eyes after their botulinum toxin. Check for natural unusual brow peaking and modify treatment doses accordingly. Pay attention to heavy male brows which often lie closer to the superior orbital rim and present a high risk of diffusion ptosis.
Keywords
Dysport, Botox, Ptosis, Scalp, Brow lift, forehead wrinkles, glabella, dermatochalasis.
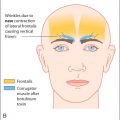
Botulinum toxin is widely known to be an excellent treatment for smoothing out both vertical and horizontal forehead lines. Patients often ask for it to be used to treat their vertical (glabellar) frown or their horizontal lines or put in a general request for improvement. It is important to find out at an early stage whether they are looking for total immobility of the forehead (this is often not possible—as explained below) or simply for a natural-looking effect with some residual forehead expression and greatly reduced wrinkles.
Forehead wrinkles are due to a combination of genetic and environmental factors, especially damage ultraviolet light. The contributions of both must be analysed when patients attend for treatment. Make sure too that they do not expect the ablation of furrows as this requires carbon dioxide laser resurfacing for maximum effect.
Older patients tend to develop deep forehead furrows from subconsciously lifting their upper lid skin and brows off the eyelids. Ptosis or blepharoplasty surgery is often accompanied by relaxation of the frontalis and elimination of such rhytids.
Botulinum toxin to the mid-forehead can lead to permanent atrophy of the muscle fibres, with an excellent long-lasting result. This usually occurs after five or six treatments at 14-week intervals. The glabellar muscles always seem to recover after treatment but can, with time, diminish in size and function. Most patients continue to return for glabellar and crow’s feet treatment, with an annual ‘top-up’ to the mid-frontalis.
Treatment of the frontalis will inevitably affect the shape of the brow. This must be assessed carefully and discussed with the patient. The treatment of horizontal lines alone may avoid changes to the brow, but once the glabella has been treated, the frontalis must be balanced with the treatment.
Remember that the shape of the brow is subject to fashion. I prefer the current trend for a female brow to have a slight arch at the junction of the medial two thirds to the lateral third. More modern trends include a horizontal brow that elevates laterally. It is essential to avoid a ‘Dr Spock’ effect with a peak to the brow, usually achieved by the unopposed action of the frontalis on the mid-brow, and most likely to occur when the glabellar muscles are treated independently.
Tell your patients what to expect from botulinum toxin at this stage, and discuss how their foreheads might alter with age. Let them know that with regular treatments, they will begin to lose their “reactive” frowning, as the central signaling area in the brain diminishes in size in response to their Botulinum toxin treatments.
Select patients as described in Chapter 6 , and take great care to avoid treating the forehead of a patient with the rare neuromuscular disorder known as chronic progressive external ophthalmoplegia (CPEO). Remember that such patients may not yet have been diagnosed. Examine the eyes and eyelids of every new patient for signs of asymmetry or abnormal muscle function. If in doubt, refer to an ophthalmologist for examination before any treatment is attempted.
CPEO is a rare neuromuscular disorder that causes total immobility of all the external ocular muscles and of the levator muscles of the eyelids. Patients eventually need an operation to attach their frontalis muscles to their eyelids (by a subcutaneous sling) so that they can open their eyes and see. The initial presentation is often a symmetrical ptosis with brow elevation.
Anatomy of frown muscles
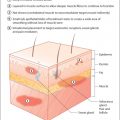
An intimate knowledge of the anatomy of the forehead is essential for successful treatment. There will always be a few patients with variations on the normal anatomy, but the typical muscle attachments are shown in Fig. 9.1 . In particular, note the following:
- ■
The frontalis muscle originates from the galea aponeurosis (near the hair line) and stretches to an insertion into the skin and the orbicularis oculi at the level of the eyebrows.
- ■
The frontalis does not cross the midline and is separated by a central muscle-free zone at the base of the nose ( Figs 9.2 and 9.3 ). Movements of the galea aponeurosis unaccompanied by movement of the frontalis will cause wrinkling of the forehead skin, especially in patients who can voluntarily ‘wiggle their ears’ or ‘move their scalp’.
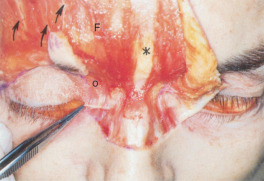
Fig. 9.2
Note that the frontalis fibres do not cross the midline. Note the paired frontalis muscles (F) with their central muscle-free zone (*). The supraorbital nerves are noted coursing upwards (small arrows) . The forceps grasp the anterior portion of the medial canthal tendon. Note the orbicularis oculi fibres (o), some of which originate from this tendon.
(From Zide, B. M., & Jelks, G. W. (1985). Surgical anatomy of the orbit . New York: Raven Press Books, Ltd. With permission of Barry Zide.)
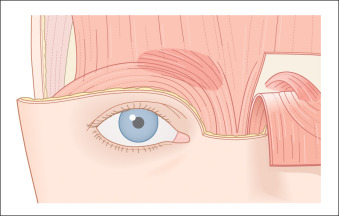
Fig. 9.3
The glabella complex. (From Zide, B. M., & Jelks, G. W. (1985). Surgical anatomy of the orbit . New York: Raven Press Books, Ltd. With permission of Barry Zide.)
- ■
The bone at the base of the nose is covered by the procerus muscle (skin attachments only), blending into the corrugator muscle at the level of the eyebrows, and the medial fibres of the orbicularis oculi below the medial part of the brow.
- ■
The corrugator muscle arises from the nasal process of the frontal bone. It is responsible for drawing the eyebrows together, creating the vertical glabellar rhytid. The corrugator lies deep to the frontalis, the procerus and the supraorbital nerves and arteries. It attaches to the skin above the medial aspect of the eyebrow.

The vertical fibres of the orbicularis oculi, which run superomedial to the medial canthal tendon, attach to the medial brow and are known as the depressor (corrugator) supercilii. The angular veins are embedded in this muscle.
Examination of brow/forehead rhytids
General appraisal
Specific glabella (vertical frown) examination
Specific forehead (horizontal frown) examination
General appraisal
Brows
Hairstyle
Ptosis
Dermatochalasis
First, examine your patient carefully and decide what botulinum toxin can do for his or her particular type of lines. Decide at this stage whether or not botulinum toxin treatment will eliminate the wrinkles. Will laser resurfacing be needed? Will the vertical lines also require a filler ( Chapter 11 )?
Eyebrows
Examine the eyebrows. Are they heavy or groomed? Some brows look as if they have descended because of their excessive growth of hair. Simple contouring of the brow with tweezers can give the illusion of a lift and instantly take years off the eyes ( Fig. 9.4 A and B). A visit to a reputable beautician may be recommended to acquire a professional shape, which the patient can easily maintain thereafter.


Hairstyle
Discuss this with the patient. If a fringe (bangs) is being worn, will the effects of botulinum toxin be noticeable? Is the patient happy to have botulinum toxin to prevent further ageing of the forehead, regardless of whether or not it can be seen? Is the patient getting a receding hairline with widow’s peaks? This can be ageing. Full forehead and scalp botulinum toxin treatment will lengthen the forehead further. They may be advised to modify their hairstyle to hide the receding areas. Has the patient seborrheic dermatitis, acne rosacea or psoriasis? In the author’s experience, this usually disappears in the zones treated with botulinum toxin, to the delight of the patients. Inform them of this possible bonus.
Ptosis
Always examine the patient for signs of ptosis (a droopy eyelid). This is common in patients over 60 years old and is usually unilateral or asymmetrical. The levator aponeurosis, which opens the eyelid, and which is also responsible for the ‘lid crease’ by its superficial insertion into the orbicularis muscle and skin, slips up under the orbital rim (and eyebrow) with age or trauma, including eye rubbing. This causes a slight drooping of the eyelid that worsens on looking down and when the patient is tired ( Fig. 9.5 A and B). Patients then compensate by tensing the frontalis muscle, developing high arched eyebrows, deep frontalis furrows and deep upper lids, which droop sleepily. The lid crease is often noticeably higher on the affected side (normal 7 to 10 millimeters, symmetrical).


In these patients, botulinum toxin to the frontalis muscle results in an immediately obvious ptosis (even though it was already present). Patients will also complain of the appearance of swollen upper lids as their brow descends. The ptosis is often asymmetrical, sometimes unilateral, and sometimes occurs in young people following trauma. It will be hard to convince these patients that the botulinum toxin did not cause the initial ptosis. Examine carefully before treating!
Basic ptosis examination
- ■
Observe the patient in the primary position (looking straight ahead).
- ■
Measure the palpebral aperture (P.A.)—the distance from the lower lash margin to the upper lash margin at the midpoint of the pupil.
- ■
Place a finger over the patient’s brow to stop it from moving.
- ■
Ask the patient to look down. Place the zero point on a fine ruler over the upper lid lashes before immediately asking the patient to look up. Now measure the point on the ruler where the lash margin has risen to.
- ■
The result is the levator muscle function (normal is 15 to 18 mms).
Dermatochalasis (eyelid bags)
The term dermatochalasis refers to age-related wrinkling and sagging of the skin over the eyelids. Examine carefully for brow elevation with overaction of the frontalis compensating for the ‘heavy skin’ and subconsciously lifting it off the lids ( Fig. 9.6 ). Botulinum treatment to the frontalis may unmask the dermatochalasis and give the illusion of ‘swelling’ of the upper lid skin ( Fig. 9.7 A and B).