Management of Facial Lacerations
John G. Fernandez
DEFINITION
Facial lacerations are a common emergency room encounter for a plastic and reconstructive surgeon.
Nearly 7 million patients require treatment for traumatic lacerations per year in the United States.1
Approximately 1.5 to 2 million patients present to the ER with facial lacerations.
According to a study by Singer et al., nearly 28% of all patients visiting the ER with lacerations had facial lacerations.2
Most complex injuries require layered closure to decrease tension and improve overall results, although single-layered closure is sufficient in small linear wounds. In select patients, topical skin adhesives are gaining acceptance.1
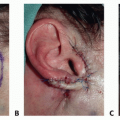
Complex wounds involving the eyelids, nose, lips, and ears may require layered closure. Facial lacerations are often associated with more severe injuries to vital structures; therefore, one needs to be suspicious of more severe underlying injuries.
Facial lacerations may involve tissue loss and may require skin undermining to achieve tension-free closure.
Composite tissue loss may require more complex reconstruction to restore lining, support, and coverage.
ANATOMY
There are several vital structures on the face that impact wound closure and/or reconstruction. These include the parotid duct, lacrimal system, white roll of the lips, eyelid margin, facial nerve, and transverse facial artery (FIG 1).
The face has an abundant blood supply and rich network of lymphatics in the dermis and subdermal areas.
PATHOGENESIS
There are many causes of facial lacerations including penetrating trauma, blunt trauma, and blast injury. Occasionally, multiple mechanisms may be present (eg, penetrating trauma in the setting of a motor vehicle accident).
The etiology of the facial laceration should be elicited in the history and physical examination; concomitant injury to musculoskeletal (eg, cervical spine injury) or soft tissues should be ruled out.
Suspicion for other injuries should be high in patients with high-speed blunt trauma and those with penetrating injuries where the entry and exit wounds are not readily identified.
Clean wounds can be repaired expeditiously. However, contaminated wounds or wounds with a significant amount of devitalized tissues may require debridement and delayed closure.
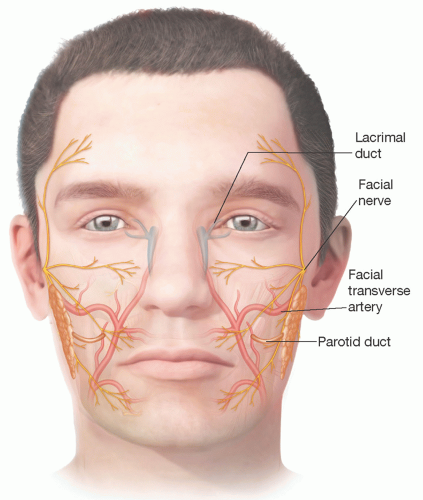 FIG 1 • Vital structures of the face. |
NATURAL HISTORY
Most routine facial lacerations that are repaired surgically heal rapidly and without difficulty.
These wounds, perhaps due to the rich vascular supply of the head and neck, rarely become infected or necrotic.
Superficial wounds that do not warrant closure heal rapidly by secondary intention often with excellent cosmetic results.
Delayed revision surgery is possible but in many cases not necessary.
Occasionally, facial lacerations, particularly those in the periorbital area, may result in prolonged swelling. This is usually managed conservatively with scar massage and, less frequently, compression.
Trapdoor scarring can occur in rounded lacerations leading to contour deformities and a noticeable scar. These scars can usually be successfully revised by undermining and occasionally with Z-plasty or W-plasty.
PATIENT HISTORY AND PHYSICAL FINDINGS
The preoperative evaluation for patients with facial lacerations includes a detailed assessment of the mechanism of injury, the etiology of the laceration and timing of injury, and the determination if loss of consciousness was associated with the trauma. In addition, physicians should:
Document timing of most recent tetanus immunization
Elicit history of keloid or hypertrophic scarring
Patient factors that may lead to wound healing complications such as diabetes, tobacco use, poor nutritional status, steroid therapy, radiation history, and immunosuppression should be documented.
Concomitant injury to the facial skeleton should be ruled out either by careful history and physical examination or with radiographic imaging as necessary. In addition, injury to other vital structures in the head and neck should be evaluated.
Significant periorbital lacerations, particularly those that occur as a result of blunt trauma or projectile injury, require funduscopic and visual acuity examination to assess for globe injury. In addition, extraocular muscle movement should be assessed, if entrapment, muscle injury, or nerve damage is suspected.
The location, size, depth of wound, tissue loss, and level of wound contamination should be assessed.
Facial nerve function and sensory changes to the skin should be evaluated. Penetrating injury to the cheek may result in laceration of the facial nerve, parotid duct, or both. Cannulation of the parotid duct and irrigation may be needed to identify the area of injury.
IMAGING
Imaging studies are not routinely necessary for assessment of simple lacerations.
If there is a suspicion of skeletal injury or injury to underlying vital structures, however, radiologic evaluation is helpful.
Noncontrast CT scans of the maxillofacial bones with thin slice axial, coronal, and sagittal views are useful for evaluating facial bone fractures.
DIFFERENTIAL DIAGNOSIS
Partial-thickness wound
Full-thickness wound
Complex soft tissue injury including bone involvement
Underlying vital structure injury
NONOPERATIVE MANAGEMENT
Healing by secondary intention is an option for superficial lesions or wounds that are contaminated.
In some cases, these wounds heal nicely and require no additional intervention.
Revision surgery, laser, or dermabrasion, and other techniques may be necessary, however, for depressed or hypertrophic scars.Related posts:
 Lateral Mandible Reconstruction With Soft Tissue Flaps
Lateral Mandible Reconstruction With Soft Tissue Flaps
 Repair of Lip Defects With Karapandzic Flaps
Repair of Lip Defects With Karapandzic Flaps
 Lower Eyelid Reconstruction With Palatal Grafts
Lower Eyelid Reconstruction With Palatal Grafts
 Reconstruction of the Ear Lobe
Reconstruction of the Ear Lobe
 Pectoralis Major Flap for Pharyngeal Reconstruction
Pectoralis Major Flap for Pharyngeal Reconstruction
 Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers
Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


