Abstract
The crow’s feet are the wrinkles at the corners of the eyes due to contraction of the orbicularis oculi when smiling. The same part of the muscle is responsible for depressing the lateral part of the eyebrows and for resting tone at the side of the orbits, ‘supporting’ the face. The inferomedial part of the orbicularis muscle also works as a pump, to draw tears in to the lacrimal system when blinking. Unwanted side effects of botulinum toxin to this area include epiphora, sagging of the lower eyelid and deepening of the nasolabial folds. Careful examination will predict unsuitable patients who, because of the shape of their bone structure and/or level of resting skin tone, would be prone to such side effects. Other treatments to the rhytids may be offered instead, such as laser resurfacing of the skin. Treatment doses may be chosen to reflect the diffusion wanted.
Keywords
Botox, Dysport, crow’s feet, orbicularis oculi, laser skin resurfacing, sun damage.
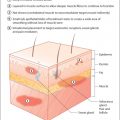
‘Crow’s feet’ are the wrinkles that form with age at the outer corners of the eyes. They are due to contraction of the orbicularis oculi muscles ( Fig. 8.1 ). Their treatment with botulinum toxin is usually straightforward, but certain aspects must be considered carefully first.
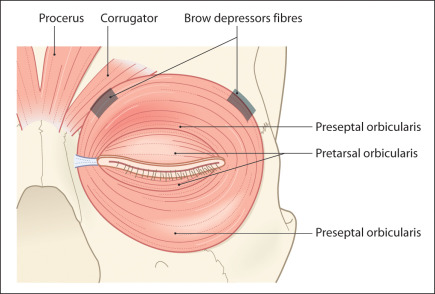
The functions of the orbicularis oculi muscle are to close the eye, to drain the tear film and to create facial expressions. Contraction of this muscle can also drag on the lateral third of the eyebrow, contributing to drooping of the brow with age. In addition, the resting tension of the orbicularis oculi muscle can increase with age and character.
Many patients keep tension at the angle constant and so have pleasant ‘smiling eyes’. This tension can be important to the appearance of the patient: it results in rhytids but also supports an ageing midface in some patients. It can also prevent the protrusion of age-related lower lid ‘bags’ (orbital fat) by supporting the orbital septum.
Injections of botulinum toxin will smooth out the rhytids and make the skin look younger, but patients may begin to look ‘thin’ around their eyes as they lose muscle bulk after repeated injections. They may also look ‘drawn’ or tired as their midface falls over the zygomatic arch. Such changes usually do not become apparent until several treatments have been undertaken. The loss of tension can reverse with time because the orbicularis muscle rarely atrophies permanently; this has been shown by the results of long-term botulinum toxin treatment of orbital blepharospasm.
This chapter covers the assessment and treatment of crow’s feet. However, it is important to reexamine patients before every treatment and to make sure that they will still look well because of it. Make certain that the botulinum toxin can do for the patient what the patient expects.
Botulinum toxin will paralyse the orbicularis muscle, making it flaccid and even atrophic. This will stop wrinkles, but the loss of muscle tone will not suit everyone.
Patient examination
Examine patients both from the front and the side.
Examine them at rest and when smiling.
Try to imagine what relaxation of their orbicularis muscle will do to their appearance.
What to look for when examining a patient
- ■
Examine the tone of the orbicularis oculi muscle and the position of rhytids. Are the wrinkles deep? Spread the skin gently between your fingers. Are they still very obvious? If they are, tell patients that they might not notice much effect from the treatment. Advise them about laser resurfacing and skin management. If the wrinkles are mild, advise patients that they might get a permanent effect with time and good skin care ( Fig. 8.2 A and B).

Fig. 8.2
One year before (A) and 1 year after (B) BOTOX to crow’s feet.

- ■
Examine the facial skin and muscle tone by asking patients to smile while pressing lightly on the zygomatic arch with two fingers ( Fig. 8.3 A and B). This stops the orbicularis muscle from contracting and so simulates the paralysis of botulinum toxin.

Fig. 8.3
(A) Press finger on zygomatic arch and ask patient to smile. This demonstrates the orbicularis muscle NOT contracting as if treated with BTX. (B) Push up skin from midface over zygoma. This demonstrates the effect of “smiling” on the midface and crows feet, independent of a BTX effect, in older skin.

- ■
Patients with severe sun damage or poor skin tone (often older patients) will observe that, on smiling, the cheek and orbicularis oculi muscles elevate the facial skin and send it into folds around the lateral orbit. Show patients that this will also happen after botulinum toxin treatment to the crow’s feet, otherwise they will think that the injections have not worked. It is often wisest not to treat such patients unless they have had surgical or laser correction of skin tone.
- ■
The Mickey Mouse sign: occasionally, patients (especially men older than 50 with good skin tone) notice that smiling causes their wrinkles to ‘bunch up’ at the level of the zygoma after treatment of their crow’s feet. This can create a curved wrinkle running from the lower orbital rim, out along the inferior border of the orbicularis oculi, over the zygomatic arch, to the top of the orbicularis oris (the Mickey Mouse smile). The periocular fibres have atrophied as planned, but the resting skin tone prevents elevation of the periocular skin and muscle on smiling. However, the excessive tone of the orbicularis oris, associated with thinning of lateral orbicularis oculi fibres, makes the smile appear much wider than the upper face. Take care with such patients.
- ■
Examine the contour of the socket. Is it shallow, allowing anterior displacement of orbital fat and bags? Does the inferior orbital rim protrude? Is it recessed behind the level of the anterior surface of the cornea? This may also be assessed by the ‘pencil test’. Ask the patient to hold a pencil vertically against the anterior cheekbone. If this passes in front of the cornea ( Fig. 8.4 A), then the patient has good lower lid skeletal support. If the pencil reaches only the lash margin (see Fig. 8.4 B), before it would penetrate the globe, then the patient is at risk of developing sagging of the lower lid and widening of the palpebral aperture if botulinum toxin is injected for pretarsal orbicularis wrinkles.

Fig. 8.4
(A) Typical bone structure means that a pencil will pass from the maxilla to in front of the cornea. (B) Some patients have a maxilla which receded from the inferior orbital rim. A pencil will pass from the maxilla through the eye. This means that inferoorbital contents (muscle and fat) are prone to bulging in front of the orbital rim, creating ‘bags’.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree