Like single-channel–type vascular malformations, combined lesions are categorized as slow-flow and fast-flow lesions. Many of the combined vascular malformations are associated with soft tissue and skeletal hypertrophy. This article discusses the diagnosis, management, and treatment of patients with capillary lymphaticovenous malformation, capillary-arteriovenous malformation, and capillary-arteriovenous fistulas and congenital lipomatous overgrowth, vascular malformations, epidermal nevi, and skeletal anomalies syndrome.
Historically, combined vascular malformations have been named after the physician who is credited with the most memorable description of the condition. Unfortunately, the eponyms are often misused and offer little insight into the underlying pathogenesis. We, therefore, favor a more anatomic description of the malformations and name them according to the anomalous vascular channels present. Like single-channel-type vascular malformations, combined lesions are also categorized as slow-flow and fast-flow lesions. Many of the combined vascular malformations are associated with soft tissue and skeletal hypertrophy.
Capillary-lymphatico-venous malformation
The first reports of patients with a slow-flow capillary-lymphatico-venous malformation (CLVM) were published in the nineteenth century by Hilaire, Trélat, and Monod. It was not until 1900 that this constellation of findings was considered more than mere coincidence. French physicians, Maurice Klippel and Paul Trénaunay, were the first to recognize Klippel-Trénaunay syndrome as a distinct entity. They proposed the main characteristics of the syndrome were a localized vascular nevus, congenital or early infantile varicosities, and hypertrophy of tissue occurring in the same body part. They also recognized the variability in the severity of symptoms. For more than 100 years, the well-worn eponym, Klippel-Trénaunay syndrome, has been used to describe patients with CLVM. It is often incorrectly called “Klippel-Trénaunay-Weber syndrome” suggesting a relation to Parkes Weber syndrome, a fast-flow malformation consisting of a capillary-arteriovenous malformation (CAVM) in association with limb hypertrophy.
Etiology and Genetics
CLVM has an equal gender distribution and occurs sporadically. No chromosomal localization or linkage with a causative gene has been identified. The pathogenesis is also not understood, but several theories have been proposed. Klippel and Trénaunay suggested that the mechanism responsible was a congenital spinal cord abnormality that altered autonomic control of capillaries causing increased blood flow to the skin, soft tissue, and bone with resultant hypertrophy. Perturbations in vasculogenesis during the specific stages of embryonic development with localized overgrowth as the hemodynamic consequence have also been theorized. The angiogenic factor gene, AGGF1 , has been suggested as a candidate susceptibility gene. Additional conjectures include paradominant inheritance, genetic mosaicism, and a polygenic hypothesis. CLVM occurring in two members of the same family has not been observed in our center.
Clinical Features
CLVM is usually diagnosed at birth. The classic presentation is an infant who presents with an enlarged lower extremity with lateral capillary malformations (CMs), lymphatic vesicles, and visible varicosities. CLVM can be suspected on antenatal imaging due to the presence of an enlarged limb. Severe cases are more likely to be detected antenatally. The diagnosis of CLVM cannot easily be confirmed until delivery since congenital lymphedema, Parkes Weber, CLOVES, and Proteus syndromes are included in the differential diagnosis.
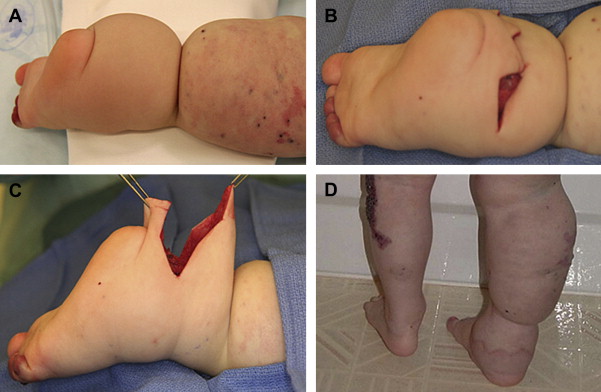
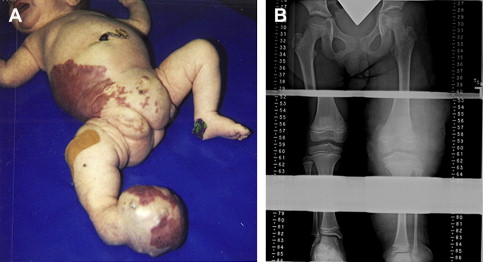
Morphologic variability is the norm in patients with CLVM ( Fig. 1 ). A single-center review of 252 patients documented involvement of the lower extremity (88%), upper extremity (29%), and trunk (23%). The deformity can range from barely perceptible capillary staining with mild soft tissue overgrowth to a grotesquely deformed limb. Soft tissue and skeletal hypertrophy of the involved limb predominate, but in 10% of patients, the affected extremity may be short or hypotrophic. Because hemihypertrophy is often a component of CLVM, many patients undergo ultrasonographic screening for Wilms tumor. Patients with CLVM, however, are not at increased risk for Wilms tumor and do not require screening.

Expansion of CLVM tends to be commensurate with the growth of the child. The CMs are often multiple, occurring predominantly on the lateral side of the extremity, buttock, or thorax. The CM is macular in a newborn and tends to darken with time. Lymphatic malformations (LMs) present as lymphedema or lymphatic cysts. Lymphatic vesicles typically erupt through the CM. LMs may be found in the buttock/perineum and in the pelvis. Bladder outlet obstruction can result from compression by the vascular malformations. The lymphatic component can also extend through the inguinal canal and into the labia or scrotum masquerading as an inguinal hernia. CLVM of the upper extremity or torso commonly involves the mediastinum or retropleural space.
Venous malformations (VMs) in CLVM are heterogeneous. They can be focal VMs, varicosities, phlebectasias, hypoplastic or aplastic vessels, or veins with absent or incompetent valves. VMs can extend into the perineum, pelvis, and retroperitoneum. VMs are also frequently encountered in the left colon and rectum. As many as 10% of CLVM patients have hematochezia. Rarely, these patients suffer chronic lower gastrointestinal tract bleeding, requiring transfusion. Colectomy, anorectal mucosectomy, and coloanal pull-through may be necessary. Rectal VMs can be associated with ectatic mesenteric veins. Portomesenteric venous thrombosis and resultant portal hypertension have been observed in patients with this pattern.
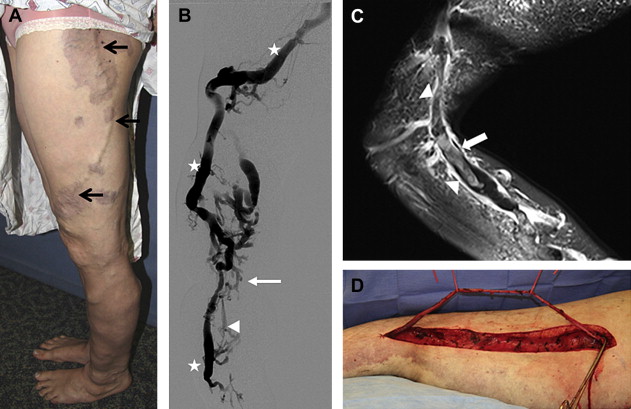
The presence of persistent embryonic veins ranges from 18% to 65% in patients with CLVM. The true occurrence is likely higher because not all patients with CLVM undergo imaging. The most common persistent embryonic vessels are the lateral marginal vein (the vein of Servelle) and the sciatic vein. Persistent embryonic vessels are often associated with hypoplasia or aplasia of the normal named branches of the deep venous system. The lateral marginal vein originates in the lateral aspect of the foot and travels proximally underneath the CM, although its course can be variable ( Fig. 2 ). The lateral marginal vein may not be visible in some patients because of soft tissue overgrowth but can be easily recognized by light palpation of a compressible cord-like structure in the lower leg and/or thigh. The lateral marginal vein is usually thick walled and incompetent; the embryonic veins can be valveless. The lateral marginal vein often has associated incompetent collateral and perforator veins, especially around the knee. Several recognized termination sites of the lateral vein include the profunda femoral, external or internal iliac, popliteal, and greater saphenous veins as well as the inferior vena cava (IVC). The persistent sciatic vein arises from the popliteal vein, or nearby tributaries, traverses the sciatic notch, and terminates at the internal iliac vein.
Soft tissue and bony hypertrophy range in severity from mild to severe. In some patients, only the subcutis is overgrown, whereas others have overgrowth of predominantly fatty tissues within or between the muscles as well. Imaging shows whether the hypertrophied components are predominantly extrafascial, intrafascial, or both. This finding is important when considering surgical debulking procedures. Bony hypertrophy may affect all bones in an extremity or can be limited to specific structures. Other limb findings seen in CLVM include macrodactyly, syndactyly, clinodactyly, polydactyly, ectrodactyly, and metatarsus varus.
Imaging
We usually do not obtain baseline imaging in asymptomatic infants with CLVM, especially in the first 6 months of life. High-quality images require anesthesia in young infants and children. We prefer to delay imaging in infants unless there is an urgent indication such as bladder outlet obstruction, severe hematochezia, or surgical planning.
Plain film radiography is used to evaluate bony deformities and to follow limb length discrepancies (LLDs). Duplex ultrasonography can help determine the presence of persistent embryonic veins as well as hypoplasia and aplasia of the deep venous system. Duplex ultrasonography provides morphologic information about the size of veins, perforators, and reflux. Because of its portability, Doppler ultrasonography can be performed as an adjunct to physical examination in the office setting. Focal VMs and LMs may be further characterized by ultrasonography. The use of ultrasonography is limited for larger lesions because of its inability to determine the exact size, extent, and tissue composition.
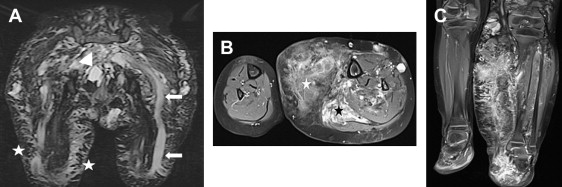
Magnetic resonance imaging (MRI) and MR venography (MRV) provide the foundation for describing type, location, and extent of the vascular malformation components of CLVM ( Fig. 3 ). Soft tissue and bony overgrowth are also depicted. Macrocystic LMs are usually seen in the pelvis and thigh, whereas microcystic LMs predominate in the abdominal wall, buttock, and distal extremity. LMs can be localized to the subcutaneous tissues or can extend into the intramuscular compartments. MRV delineates the extremity veins and demonstrates the anomalous venous channels. The veins of the trunk, pelvis, rectum, and mesentery are readily shown by MRV. MR arteriography is not useful because the arteries are normal in CLVM.
Venography may be useful for mapping the venous drainage and delineating malformations during sclerotherapy (see Fig. 2 ). It can be difficult to opacify the deep venous system with this technique because contrast preferentially flows into the capacious superficial channels. The use of tourniquets, direct puncture, ascending and descending phelobography, and dependency optimizes visualization. Venography is generally performed only when an intervention is planned to avoid unnecessary morbidity.
Special Issues
A team of specialists is often necessary to manage patients with CLVM. Some of the more common manifestations of this disease include superficial thrombophlebitis, deep venous thrombosis (DVT), pulmonary thromboembolism (PE), infection, pain, and depression. Parental and patient education should start in infancy and continue into adulthood.
Persistent embryonic and phlebectatic veins can be troublesome to patients. These veins can be associated with pain, edema, sensation of heaviness, bleeding, and ulceration. Superficial thrombophlebitis has a frequency between 15% and 50%. The organized thrombus may calcify and form phleboliths which can be a source of discomfort. Treatment consists of non-narcotic analgesics, anti-inflammatory medications, and limb elevation. Low-dose aspirin (81 mg) can be used to minimize phlebothromboses. If phlebothromboses recur, sclerotherapy can be considered.
DVT and PE occur in 4% to 11% of cases of CLVM. Persistent embryonic veins are likely the major source. Flow in these capacious channels is often retrograde or stagnant; thrombosis occurs due to diminished flow. Because these channels may connect anomalously to the femoral or iliac veins or IVC, a dislodged clot may result in PE. Patients with anomalous connections to the femoral or iliac veins or IVC should be considered for pre-emptive ablation or resection to decrease the risk of DVT and PE. This pattern should also be recognized before major invasive procedures, and when present, we recommend the placement of retrievable IVC filters. Careful pre-placement mapping of the venous drainage of the involved extremities is imperative to ensure that the drainage does not bypass the site of filter placement. In addition, treatment with perioperative prophylactic anticoagulation is recommended in all patients with CLVM. Our general practice is to administer low-molecular-weight heparin (LMWH) preoperatively for 14 days and to continue postoperatively until the patient has returned to full mobility.
Some patients with CLVM, particularly those with an extensive VM component or large embryonic veins, may have altered coagulation profiles due to constant activation of the coagulation cascade. Stagnant blood leads to the production of thrombin and conversion of fibrinogen to fibrin. Fibrinolysis results in elevated levels of fibrin degradation products. These products are measured with D-dimer levels. This process is called localized intravascular coagulopathy. We obtain a baseline coagulation profile (platelet count, prothrombin time, partial thromboplastin time, fibrinogen, and D-dimer level) before any major procedure. LMWH should be administered to those patients with elevated D-dimer levels perioperatively to stabilize their hematologic status.
CLVM patients are susceptible to infection. Chronic lymphedema, poor skin integrity, venous stasis, and open lymphatic vesicles, especially when located on the lower leg or foot, predispose patients to cellulitis. Excellent skin hygiene and proper shoes are essential. Perineal and pelvic involvement also increases the risk of complications. Some patients may present with recurrent bacteremia due to translocation from gut flora. Patients with recurrent cellulitis may require antibiotic prophylaxis.
Chronic pain and depression should not go unrecognized. Pain is a major complaint in 88% of patients. Varicosities, VMs, and ectatic embryonic veins contribute to venous stasis in the affected extremity. Patients report that their legs often ache and feel heavy. Intra-articular vascular malformations are also a source of pain. Multiple factors, such as chronic pain, frequent hospitalizations, and feelings of isolation, contribute to the development of depression. School-aged children and adolescents may be ostracized by their peers because of visible deformities and physical limitations.
Orthopedic consultation is usually necessary to evaluate the need for extremity amputation, management of intra-articular disease, and LLD. Amputation is indicated for lower extremity deformities that would preclude ambulation ( Fig. 4 ). The level of amputation depends on the extent of the deformity. Gross foot enlargement that impairs ambulation and the ability to wear shoes requires orthopedic corrective procedures and partial amputations. It is preferable to perform these procedures during infancy. In some instances, VMs have an intra-articular extension, most commonly in the knee joint. Range of motion may be limited because of the pain resulting in the development of flexion contractures. VMs may also cause hemarthroses, arthropathy, and ultimately arthritis. Focused imaging of the joint may show synovial involvement. Sclerotherapy can reduce pain and improve mobility. Simultaneous arthroscopy can be performed to clarify the extent of intra-articular involvement. Subsequent synovectomy may prevent recurrent pain, hemarthrosis, and premature arthritis.
LLD is common in CLVM, occurring in 67% of patients. The average LLD in CLVM is 1.75 cm, ranging from 0.1 to 10.0 cm. The initial assessment should start in infancy. The infant is placed supine on a flat surface, the feet are held in place, and the knees are flexed to 90°. Determination of whether the femur or tibia of the affected limb is longer or shorter can be made in this position. Older patients should be evaluated while standing on a flat floor. Symmetry of the gluteal folds and transverse popliteal skin creases of both legs should be inspected. Suspicion of a LLD warrants radiographic assessment. A standing or supine anteroposterior radiograph of both lower extremities is obtained. Alternatively, a scanogram can be taken in the supine position with a ruler placed between the lower extremities. The hips, knees, and ankles are evaluated (see Fig. 4 ). Regardless of the method, it should be consistent to allow for comparison.
Prediction of LLD in patients with complex combined vascular malformations is challenging. Yearly orthopedic examination to evaluate bone age helps to determine the most appropriate time for corrective orthopedic procedures. Differences less than 0.5 cm require no therapy. Differences between 0.5 and 2.0 cm are managed with internal or external heel lifts. Discrepancies greater than 2 cm in the legs are often treated with epiphysiodesis at the distal femoral and/or proximal tibial growth plates around 11 to 12 years of age. It is not necessary to correct upper extremity LLD.
Nonoperative Management
Compression therapy is the mainstay of conservative treatment in patients with CLVM. We generally do not recommend compression therapy until the child begins to walk; compression is difficult in toddlers, and garments are expensive. Elastic bandages can be used during periods of rapid growth. We recommend routine use of compression therapy by 4 to 5 years of age to minimize swelling from lymphedema, chronic venous insufficiency, and lymphatic vesicles. Compression therapy may improve pain and the sensation of heaviness. The length of the garment depends on the extent of extremity involvement. The greatest tolerated pressure should be used (a good starting point is 30–40 mm Hg). Pneumatic compressive devices are also an option, especially while recumbent or sleeping.
Sclerotherapy is used to treat focal VMs, small varicosities, LMs, and lymphatic vesicles. Small focal VMs can be accessed by direct puncture with injection of the sclerosant under fluoroscopy. Manual compression or tourniquets are used to limit venous drainage and systemic delivery of the sclerosant. Chronic venous stasis ulcers may improve or heal after sclerotherapy. Microfoam sclerotherapy for the treatment of large VMs and phlebectasias has increased in popularity in recent years, and several studies have documented improvement in pain and reduction in the size of the malformation. The delivery of the sclerosant in microfoam form allows for more precise dosing and prolongs contact time with the endothelial surface. Regardless of the sclerosing agent chosen (alcohol, sodium tetradecyl sulfate, polidocanol), multiple sclerotherapy sessions are often required. Macrocystic LMs can also be treated with sclerotherapy. Cutaneous lymphatic vesicles may be managed with intravesicular sclerotherapy, cauterization, carbon-dioxide laser ablation, or excision.
Early detection of persistent embryonic veins allows for intervention to prevent chronic venous insufficiency, pain, DVT, and PE. Identification of patients with persistent embryonic vessels by a combination of physical examination, screening ultrasonography, and MRI/MRV should be performed in the first five years of life. We recommend that consideration be given to obliteration or removal of persistent embryonic veins with anomalous connections to femoral or iliac veins or the IVC in early childhood because of the risk of DVT and PE (see Fig. 2 ). Endovenous laser ablation (EVLA) is a minimally invasive procedure for the obliteration of persistent embryonic veins of suitable size. Recanalization or recurrent reflux rates of 67% have been observed when the venous diameter is greater than 1.2 cm. The vessels are smallest in childhood and are therefore more amenable to EVLA. Older patients are often not candidates for EVLA because the vessel is too large; hence, it must be resected. Historically, many practitioners have been reluctant to consider surgical excision of the lateral marginal vein when associated with hypoplasia or aplasia of the deep venous system. They feared that removal of the vein would prevent venous outflow from the leg resulting in phlegmasia alba or cerulea dolens. We support prior observations that the lateral marginal vein can be safely removed in the presence of hypoplasia because the hypoplastic veins dilate spontaneously to an almost normal size. This rerouting of venous flow also occurs when the lateral marginal vein is ablated or resected in the face of an aplastic deep venous system.
Operative Treatment
Debulking procedures to remove excess girth traditionally have not been recommended due to the possibility of long-term complications from fibrosis and pedal edema. On the contrary, our experience with surgical debulking has been positive. We believe that surgical debulking can be performed safely with minimal long-term morbidity. There is tremendous psychological value for both the patient and family in making a child with CLVM look as “normal” as possible. In our center, debulking is considered to reduce excessive bulk and weight of the lower extremity, trunk, perineum, buttock, and genitalia. Debulking also can benefit those patients with a history of multiple soft tissue infections. The most important factor in deciding whether or not a patient is a candidate for surgical debulking of the extremity is the location of the overgrowth (see Fig. 3 ). We do not recommend debulking of intrafascial overgrowth due to morbidity associated with muscle resection and possible injury to neurovascular structures.
Surgeons must be committed to managing all postoperative complications and to reoperating when necessary. Patients are counseled about the risks of DVT, PE, injury to neurovascular structures, possible need for blood transfusion, and prolonged use of closed suction drains. There is a high likelihood of wound dehiscence, flap necrosis, and infection; the skin flaps are composed of abnormal skin with poor lymphatic drainage and altered circulation. Postoperatively, lymphatic vesicles may appear in or around the scar. We also inform patients about the potential need for multiple-staged resections, especially when the overgrowth is circumferential and extensive.
Because of significant morphologic variation in the presentation of CLVM, each patient’s debulking procedure is tailored based on problematic areas. After appropriate counseling and administration of perioperative anticoagulants when indicated, the surgeon must decide which portion of the extremity to debulk. In general, we recommend starting the procedure in the most extensive area; there usually is disproportionate overgrowth of the lateral leg. Some patients have excess soft tissue around their ankle which can make fitting into shoes difficult ( Fig. 5 ). Debulking the ankle can be done alone or in combination with a more extensive procedure. Tourniquets may be used when performing a distal extremity operation to minimize blood loss. The use of an intraoperative cell salvage machine can limit blood transfusions.