This article describes the clinical features, diagnosis, and management of arteriovenous malformation, capillary malformation–arteriovenous malformation, and PTEN-associated vascular anomaly.
Arteriovenous malformation (AVM) results from an error in vascular development during embryogenesis. An absent capillary bed causes shunting of blood directly from the arterial to venous circulation through a fistula (direct connection of an artery to a vein) or nidus (abnormal channels bridging the feeding artery to the draining veins). AVM may develop because primitive arteriovenous shunts fail to undergo apoptosis; AVM is 20 times more common in the central nervous system, where apoptosis is rare. Genetic abnormalities cause certain types of familial AVMs. Hereditary hemorrhagic telangiectasia is attributable to mutations in endoglin and activin receptor–like kinase 1 (ALK-1), which affect transforming growth factor-beta (TGF-β) signaling. Capillary malformation–arteriovenous malformation (CM-AVM) results from a mutation in RASA1. Patients with PTEN mutations also can develop arteriovenous anomalies.
Arteriovenous malformation
Clinical Features
The most common site of extracranial AVM is the head and neck, followed by the limbs, trunk, and viscera. Although present at birth, AVM may not become evident until childhood. Lesions have a pink-red cutaneous stain, are warm, have a palpable thrill or bruit, and may be initially mistaken for a capillary malformation or hemangioma. Arteriovenous shunting reduces capillary oxygen delivery causing ischemia; patients are at risk for pain, ulceration, bleeding, and congestive heart failure. AVM also may cause disfigurement, destruction of tissues, and obstruction of vital structures. High-pressure shunting of blood can cause venous hemorrhage, and rupture of arteries may occur in weakened areas, such as aneurysms. Arterial bleeding most commonly occurs at skin or mucosal surfaces from erosion into a superficial component of the lesion.
Although AVM is considered a quiescent lesion, as evidenced by endothelial turnover, it is not a static malformation; it progresses over time and recurs after treatment. Although the presence of an AVM may be troublesome, it is the expansion of the lesion that is the primary cause of morbidity. AVM worsens over time, and can be classified according to the Schobinger staging system ( Table 1 ). AVM may enlarge because of increased blood flow causing collateralization, dilatation of vessels (especially venous ectasia), and thickening of adjacent arteries and veins. Latent arteriovenous shunts may open, stimulating hypertrophy of surrounding vessels from increased pressure. Alternatively, aneurysms may increase the size of these lesions.
| Stage | Clinical Findings |
|---|---|
| I (Quiescence) | Warm, pink-blue, shunting on Doppler |
| II (Expansion) | Enlargement, pulsation, thrill, bruit, tortuous veins |
| III (Destruction) | Dystrophic skin changes, ulceration, bleeding, pain |
| IV (Decompensation) | Cardiac failure |
Angiogenesis (growth of new blood vessels from preexisting vasculature) and/or vasculogenesis (de novo formation of new vasculature) may be involved in AVM expansion. Although neovascularization may be a primary stimulus for AVM growth, it also could be a secondary event. For example, ischemia, a potent stimulator of angiogenesis, causes enlargement of AVM after proximal arterial ligation or trauma. Alternatively, increased blood flow because of arteriovenous shunting may promote angiogenesis; vascular endothelial growth factor (VEGF) production and endothelial proliferation are stimulated by elevated blood flow. Because both males and females have a twofold risk of progression to a higher Schobinger stage in adolescence, circulating hormones during this period may promote AVM expansion.
Diagnosis
Ninety percent of AVMs are diagnosed by history and physical examination. Unlike hemangioma, AVM expands after infancy, and, in contrast to capillary malformation, AVM has fast-flow. Hand-held Doppler examination showing fast-flow aids the clinical diagnosis and can exclude slow-flow vascular anomalies, such as venous or lymphatic malformation. If AVM is suspected, the diagnosis can be confirmed by ultrasonography (US), with color Doppler examination showing fast-flow and shunting. Magnetic resonance imaging (MRI) also is obtained to (1) confirm the diagnosis, (2) determine the extent of the lesion, and (3) plan treatment. To adequately assess a vascular anomaly, MRI with contrast and fat suppression, as well as T2-weighted sequences, is necessary. MRI shows dilated feeding arteries and draining veins, enhancement, and flow-voids. Unlike hemangioma, AVM does not have a significant parenchymal mass. If the diagnosis remains unclear after US and MRI, angiography is performed. Angiography also is indicated if embolization or resection is planned, and can help determine the flow dynamics of the lesion. AVM shows tortuous, dilated, arteries with arteriovenous shunting and enlarged draining veins on angiography. The nidus is angiographically manifest as dysplastic, tortuous, small vessels, with occasionally ill-defined larger contiguous vascular spaces. Computed tomography (CT) may be indicated if the AVM involves bone. Histopathological diagnosis of AVM is rarely necessary, but may be indicated if imaging is equivocal or to rule out malignancy. Biopsy of an AVM may be complicated by bleeding and reactive expansion of the lesion.
Nonoperative Management
For superficial AVMs, patients should apply hydrated-petroleum to prevent desiccation and subsequent ulceration. Compression garments for extremity lesions may reduce pain and swelling, but can also worsen symptoms. If bleeding occurs, it is readily controlled by compression; further intervention is rarely necessary. Because estrogen is proangiogenic and may stimulate AVM progression, we recommend progesterone-only oral contraceptives. Although pregnancy has been thought to increase the risk of AVM expansion, pregnant women with Stage I lesions do not have an increased rate of progression compared with nonpregnant women. However, pregnancy in women with Stage II–IV AVM has not been studied, and thus we caution women with advanced lesions that pregnancy may exacerbate their malformation.
Operative Management
Indications
Approximately three-fourths of patients with AVM require treatment in childhood or adolescence; the remaining individuals do not need intervention until adulthood. Because AVM is often diffuse, involving multiple tissue planes and important structures, cure is rare. The goal of treatment usually is to control the malformation. Intervention is focused on alleviating symptoms (ie, bleeding, pain, ulceration), preserving vital functions (ie, vision, mastication), and improving a deformity. Management options include embolization, resection, or a combination; pharmacologic treatment currently does not exist. Resection offers the best chance for long-term control, but the reexpansion rate is high and extirpation may cause a worse deformity than the malformation. Embolization is not curative, and most AVMs will ultimately reexpand after embolization. Consequently, embolization is most commonly used preoperatively to reduce blood loss during resection, or for palliation of unresectable lesions.
Asymptomatic AVM should be observed unless it can be removed for possible cure with minimal morbidity; embolization or incomplete excision of an asymptomatic lesion may stimulate it to enlarge and become problematic. Intervention is determined by (1) the size and location of the AVM, (2) the age of the patient, and (3) Schobinger stage. Although resection of an asymptomatic Stage I AVM offers the best chance for long-term control or “cure,” intervention must be individualized based on the degree of deformity that would be caused by excision and reconstruction. For example, a large Stage I AVM in a nonanatomically important location (ie, trunk, proximal extremity) may be resected without consequence, before it progresses to a higher stage when excision is more difficult and the recurrence rate is greater. Similarly, a small, well-localized AVM in a more difficult location (ie, face, hand) may be removed for possible “cure” before it expands and complete extirpation is no longer possible.
In contrast, a large, asymptomatic AVM located in an anatomically sensitive area, such as the face, is best observed, especially in a young child not psychologically prepared for a major procedure. First, resection and reconstruction may result in a more noticeable deformity or functional problem than the malformation. Second, although the recurrence rate is lower when a Stage I AVM is resected, it is still high and thus even after major resection and reconstruction the malformation may recur. Third, some children (17.4%) do not experience significant long-term morbidity from their AVM until they are adults.
Intervention for Stage II AVMs is similar to Stage I lesions. However, the threshold for treatment is lower if an enlarging lesion is causing a worsening deformity or if functional problems are expected. Stage III and IV AVMs require intervention to control pain, bleeding, ulceration, or congestive heart failure.
Embolization
Embolization involves the delivery of an inert substance, typically through a catheter proximal to the AVM, to occlude blood flow and/or fill a vascular space. Successful embolization requires penetration of the embolic agent to the nidus, ideally to the point of initial venous drainage. Proximal arterial embolization is contraindicated because recanalization occurs and the lesion becomes inaccessible for future embolization.
In addition to the replacement of arterialized blood with an inert embolic substance, ischemia and scarring may further reduce arteriovenous shunting, shrink the lesion, and improve symptoms. Even if significant volume reduction does not occur after embolization, symptoms are improved. For the vast majority of patients, embolization is performed under general anesthesia. Often multiple treatments are required, typically spaced by several weeks.
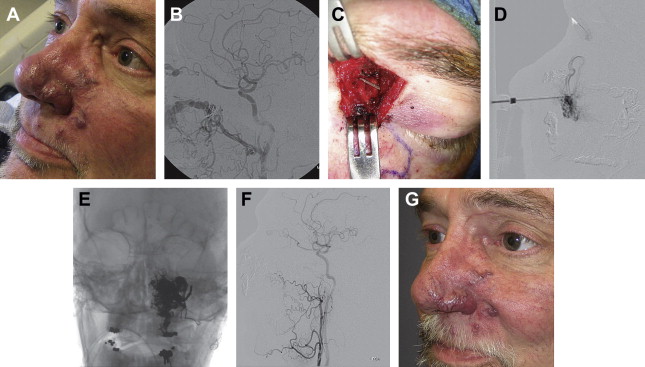
Because the AVM is not removed, almost all lesions eventually will expand after treatment; most older studies suggest that multiple embolizations do not lower the rate of recurrence, although newer embolic agents may offer more lasting results. Stage I AVM has a lower recurrence rate than higher-staged lesions. Most recurrences occur within the first year after embolization and 98% reexpand within 5 years; although this may reflect results obtained with older embolic agents. Patients who have not exhibited enlargement 5 years following embolization are more likely to have long-term control. Despite the high likelihood of reexpansion, embolization can effectively palliate an AVM by reducing its size, slowing expansion, and alleviating pain and bleeding ( Fig. 1 ). The aim of preoperative embolization is to reduce blood loss during extirpation.
Substances used for embolization may be liquid (n-butyl cyanoacrylate [n-BCA], Onyx, ethanol) or solid (polyvinyl alcohol [PVA] particles, coils). The choice of embolic agent depends on whether embolization is being used as primary treatment or as a preoperative adjunct to excision. For preoperative embolization, temporary occlusive substances (gelfoam powder, PVA, embospheres), which may undergo phagocytosis if left in place over several weeks, are used. Delivery of PVA and embospheres with different particle sizes allows the initial occlusion of small, distal vessels followed by blockage of more proximal branches with larger emboli. Permanent liquid agents capable of permeating the nidus (ethanol, n-BCA, Onyx) are used when embolization is the primary treatment. We prefer Onyx, which is an ethylene-vinyl alcohol copolymer (EV3 Neurovascular, Irvine, CA, USA). Onyx precipitates on the surface after contact with blood. A nonadhesive liquid core is maintained, which allows repetitive injection from the same pedicle, each time filling a different AVM compartment. Consequently, Onyx allows more aggressive embolization than other liquid agents of multiple nidal areas from a single catheter position. Onyx also causes less inflammation and endothelial damage than n-BCA or alcohol, and resection is facilitated because the vessels are less fragile.
The most frequent complication of embolization is ulceration, which is more common for superficial lesions. Wounds are allowed to heal secondarily with local wound care. Distal migration of embolic material can cause ischemic injury to uninvolved tissues. Unlike sclerotherapy for slow-flow malformations, posttreatment edema after AVM embolization is rare, unless ethanol is used as the embolic agent. Except for small lesions, most patients are observed overnight in the hospital. If swelling is a significant concern, dexamethasone can be administered perioperatively followed by a 1-week oral corticosteroid taper. Posttreatment swelling may necessitate close monitoring if airway or orbital lesions are embolized; deep extremity lesions are at risk for compartment syndrome. Patients and families are counseled that AVM is likely to reexpand following treatment, and thus additional embolizations may be required in the future.
Sclerotherapy
Sclerotherapy involves the transcutaneous injection of a substance into the malformation, which causes endothelial destruction and thrombosis. Subsequent fibrosis of the vascular space decreases the size of the lesion and improves symptoms. Sclerotherapy is reserved for an AVM that cannot be accessed transarterially, usually because of previous embolization of proximal feeding vessels. Alternatively, a localized AVM may be treated by sclerotherapy as well. The danger in using sclerosants in a high-flow lesion is the potential for the agent to escape into the systemic circulation. Our preferred sclerosants are sodium tetradecyl sulfate (STS) and absolute ethanol. Although ethanol is more effective than STS, it has a higher complication rate. Because ethanol can cause nerve damage, it should be used with great care in proximity to important structures (ie, facial nerve), and the dose should not exceed 1 mL/kg (maximum of 60 mL).
Resection
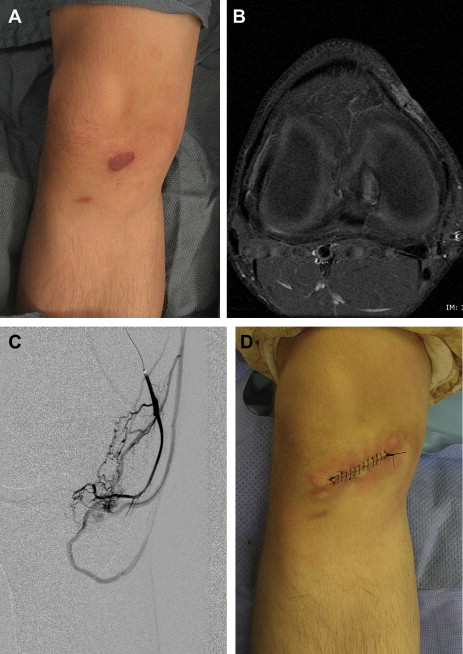
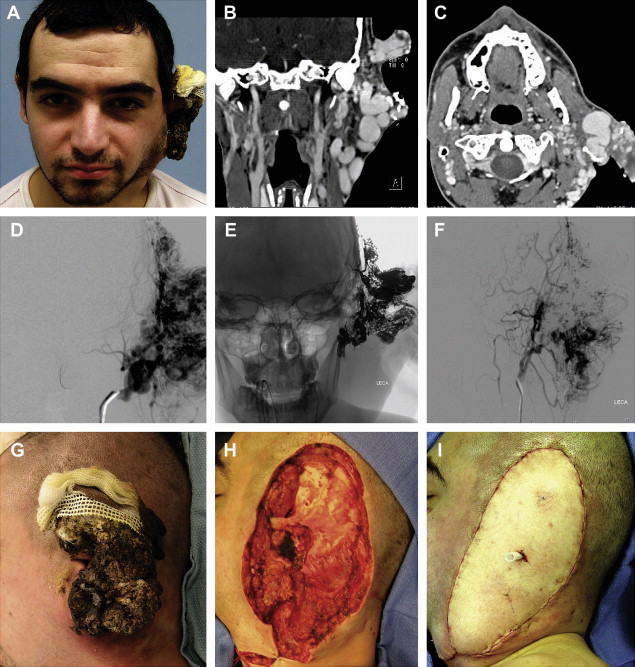
Resection of AVM has a lower recurrence rate than embolization and is considered for well-localized lesions ( Fig. 2 ) or to correct focal deformities (ie, bleeding or ulcerated areas, labial hypertrophy) ( Figs. 3 and 4 ). Wide extirpation and reconstruction of a large, diffuse AVM should be exercised with caution because (1) cure is rare and the recurrence rate is high; (2) the resulting deformity is often worse than the appearance of the malformation; and (3) resection is associated with significant blood loss, iatrogenic injury, and morbidity.
Related posts:
 Vascular Anomalies: Current Overview of the Field
Vascular Anomalies: Current Overview of the Field
 Pathogenesis of Vascular Anomalies
Management of Lymphatic Malformations
Management of Venous Malformations
Pathogenesis of Vascular Anomalies
Management of Lymphatic Malformations
Management of Venous Malformations
 Management of Combined Vascular Malformations
Management of Combined Vascular Malformations
 Special Considerations in Vascular Anomalies: Operative Management of Craniofacial Osseous Lesions
Special Considerations in Vascular Anomalies: Operative Management of Craniofacial Osseous Lesions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


