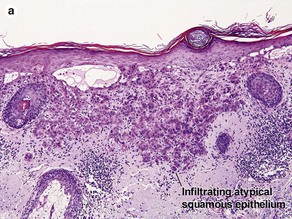
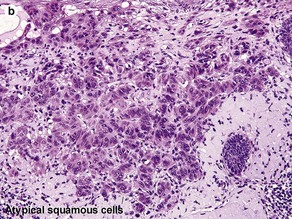
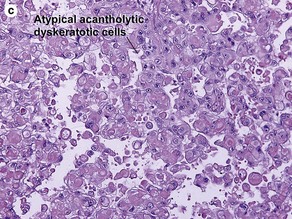
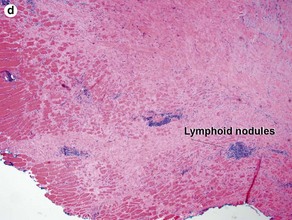
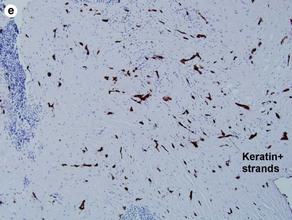
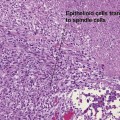
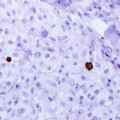
Chapter 3 The malignant keratinocytes of Bowen’s disease can keratinize and become part of the stratum corneum. In contrast, the malignant cells of Paget’s disease or melanoma often “spit out” into the stratum corneum intact. Bowen’s disease contains glycogen and is periodic acid-Schiff (PAS) positive and diastase sensitive. In contrast, Paget’s disease contains sialomucin and is PAS positive, diastase resistant. Bowen’s disease is negative for carcinoembryonic antigen (CEA) whereas Paget’s stains for CEA. Ducts and sebaceous differentiation distinguish porocarcinoma and sebaceous carcinoma. Fig 3-10 (a,b) Well-differentiated invasive squamous cell carcinoma. (c) Acantholytic squamous cell carcinoma. (d,e) Desmoplastic squamous cell carcinoma (H&E and keratin 907 immunostain)
Malignant tumors of the epidermis
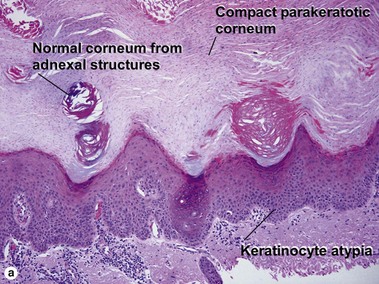
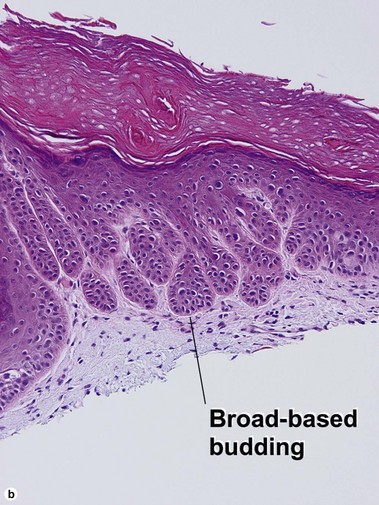
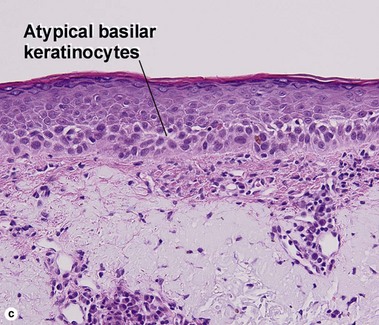
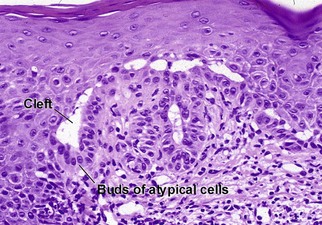
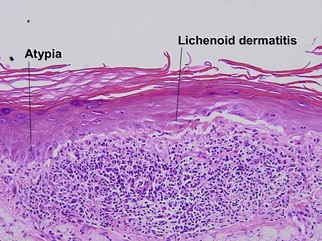
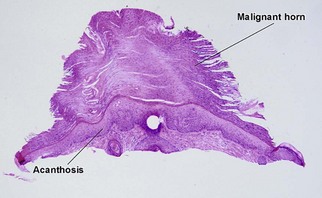
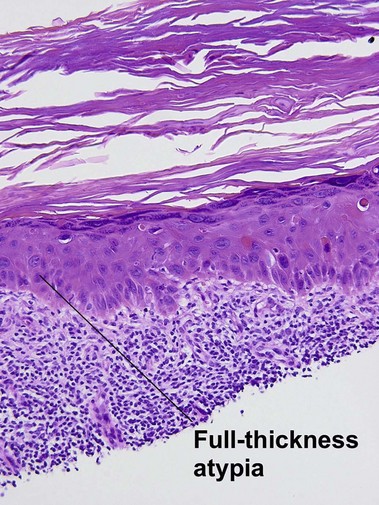
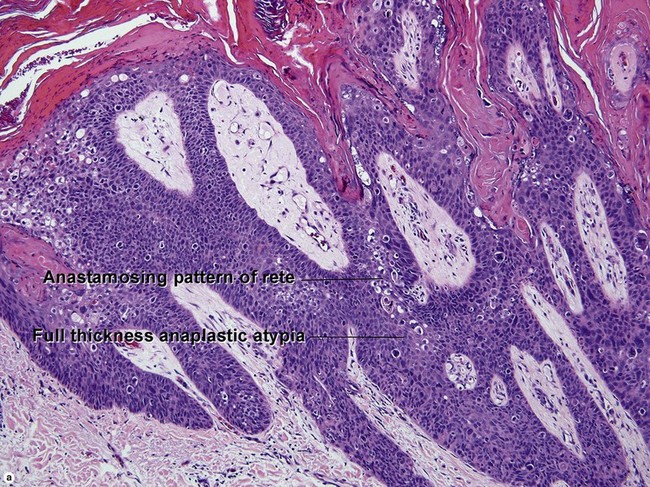
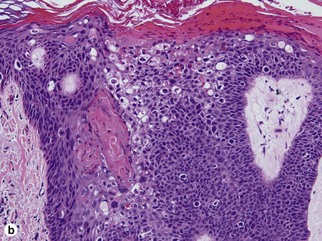
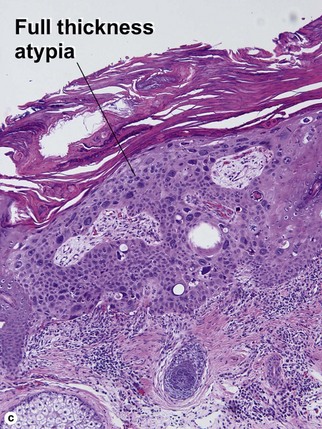
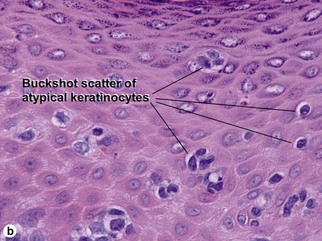
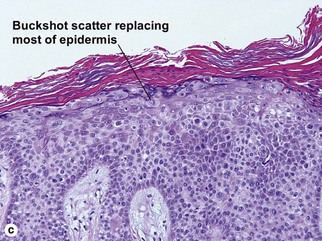
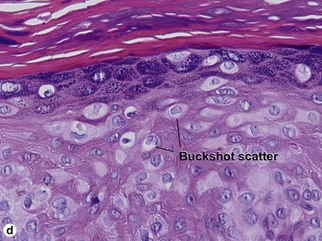
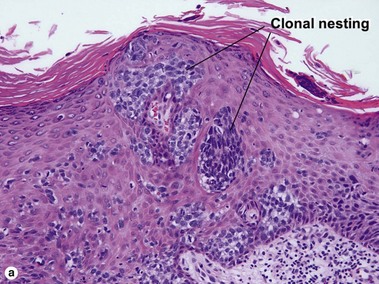
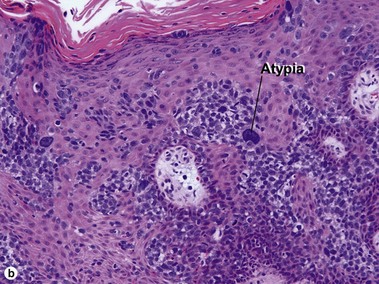
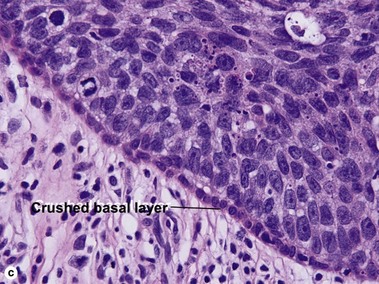
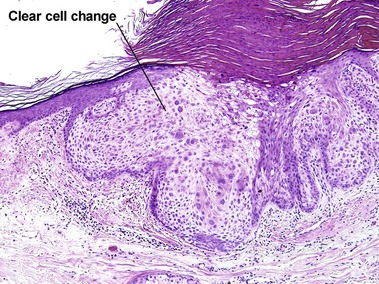
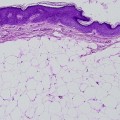
Bowen’s disease
Squamous cell carcinoma