Lower Lip Reconstruction With the Nasolabial Flap
George Xipoleas
Matthew S. Kilgo
DEFINITION
The nasolabial flap is a versatile random pattern superiorly or inferiorly based flap that can be used to reconstruct defects of the lower lip.1,2,3
The nasolabial flap can be used to reconstruct defects spanning the entire transverse dimension (approximately 7 cm) of the lip.
In most cases, the flap can be used to reconstruct the entire vertical dimension (approximately 2.0 cm) of the lower lip.
ANATOMY
The lower lip is composed of the intraoral mucosa, vermilion, and skin/subcutaneous tissue extending inferiorly to the labiomental fold.
The most distinguishing feature of the lip is the vermilion, a modified mucosa that covers the free margin of the lip and is adapted to external exposure.
There are relatively few salivary glands beneath the vermilion in contrast to the mucosa.
Musculature of the lower lip (FIG 1A)
The body of the lower lip is predominantly composed of the orbicularis oris.
The primary muscle responsible for oral competence. It compressed and protrudes the lips and creates the oral sphincter.
The orbicularis oris muscle has two points of origin.
The peripheral fiber originates from the modiolus where they interdigitate with the fibers of the adjacent muscles of facial expression (buccinators, levator anguli oris, depressor anguli oris, levator labii superioris, depressor labii inferioris, zygomaticus minor, and zygomaticus major). This is considered the peripheral portion of the muscle.
The central fibers are restricted to the lip proper and are considered the labial portion of the muscle.
The muscle fibers interdigitate in the midline and insert into the mucosa.
The mentalis muscle elevates and protrudes the lower lip.
Originates from the incisive fossa of the mandible
Inserts into the skin of the chin
The depressor labii inferiors muscle draws the lower lip downward and laterally.
It originates from the mandible adjacent to the mental foramen.
It inserts into the skin of the lower lip.
Innervation of the lower lip (FIG 1B):
Motor innervation to the lower orbicularis oris is from the marginal mandibular and buccal branches of the facial nerve.
Motor innervation to the depressor labii inferioris and mentalis is from the marginal mandibular branch of the facial nerve (cranial nerve 7).
Sensory innervation of the lower lip is from the mental branch (V3—third division) of the trigeminal nerve (cranial nerve 5).
Blood supply of the lower lip (FIG 1C):
Paired lower labial arteries that are branches of the facial artery
They course horizontally across the lip in the submucosal plane, posterior to the orbicularis muscle at approximately the same level as the anterior vermilion line.
Lymphatic drainage (see FIG 1C):
Drainage occurs via the submandibular and submental lymph nodes.
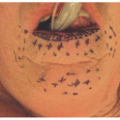
The nasolabial crease is an anatomic landmark created by the insertion of the superficial muscular aponeurotic system (SMAS) into the skin junction of the cutaneous lip and the cheek.
Marks the division of the cheek lateral to the fold and the lip and nose medial to the fold
Medial to the crease, the skin of the lip is tightly attached to the orbicularis oris muscle.
Lateral to the crease, the skin of the cheek is loosely attached to the deep muscular fascia, and there is an abundance of subcutaneous tissue and skin laxity.
PATHOGENESIS
The majority of lip defects in adults are secondary to excision of malignant tumors. Other causes of lip defects include vascular malformations, congenital defects, and trauma.
Neoplasms of the lip are primarily related to actinic changes.
Upward of 90% of lower lip neoplasms are squamous cell carcinomas (SCCs) with the remainder being made up of basal cell carcinomas (BCCs), salivary gland carcinomas, and melanomas.
PATIENT HISTORY AND PHYSICAL FINDINGS
A detailed history and physical examination are important to determine the type of lesion and intervention.
The physical examination should be directed not only to the lips but to the oral mucosa and to the lymphatic drainage basins, ie, the submandibular and submental nodes.
What is the patient’s age, sex, and skin type?
Cancers of the lip are most common in lighter skin males in their sixth decade. There is a 6:1 ratio of SCC in males to females.Related posts:
 Mandible Reconstruction With Fibula Flap With Templates
Mandible Reconstruction With Fibula Flap With Templates
 Repair of Lip Defects With Karapandzic Flaps
Repair of Lip Defects With Karapandzic Flaps
 Lower Eyelid Reconstruction With Palatal Grafts
Lower Eyelid Reconstruction With Palatal Grafts
 Reconstruction of the Ear Lobe
Reconstruction of the Ear Lobe
 Pectoralis Major Flap for Pharyngeal Reconstruction
Pectoralis Major Flap for Pharyngeal Reconstruction
 Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers
Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


