The goal would be similar to Caucasian patients in that all patients would like to have maximum improvement with minimal detectability of the surgical procedure. With regard to scars, the incisions must be no longer than necessary to accomplish the desired goal, and should be carefully placed so that color matches are ideal and there is no objectionable hair shift. In addition, the technique of making an incision for male patients should be made so that hairs will grow through the scars whenever possible. For non-Caucasian patients it is essential that attention be made to all of the known details and techniques, to avoid detection that surgery has been performed.
It is now possible for refinement of the details concerning the diagnosis of face and neck problems, along with the ability to restore a natural appearance 15 or 20 years younger with minimal detectability of surgical incisions.
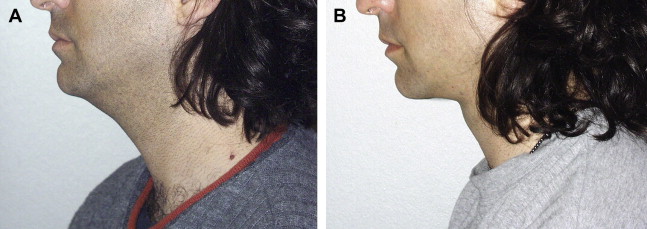
Incision placement
Incisions should only be as short or long as needed to produce the desired results ( Fig. 1 ). In all non-Caucasian patients ( Fig. 2 ), the careful placement of the incision within the first color change from the cheek to the helix of the ear almost always results in a nondetectable scar, whereas if that location is anterior by 3 or 4 mm there will be a visible scar because one would see a color change, the scar, another color change, and still another color change. This common error has been noted by the author in non-Caucasians as well as Caucasians who have much redness to their skin. The chances of a nondetectable scar placed along the edge or margin of the helix is almost always undetectable, whereas a scar placed on the tragus or anterior to the tragus frequently results in a change in pigmentation or a change in color match of the cheek skin to the tragus skin, which makes it obvious that the person has had a facelift from across the dining table and frequently even from across the room.

For a nonoperated appearance the earlobe should have a transition from the earlobe as a pedicle of skin, so that there is not a scar at the junction of the earlobe with the thick cheek skin. In the postauricular area in both Caucasians and non-Caucasians, incisions along the hair have much less possibility of creating a visible problem with alopecia caused by hair shift than making the incision above the occipital hair. An exception to this would be for neck corrections in patients who have no skin to be discarded because the excessive neck skin goes into the concavity formed by the new neck contour (see Fig. 1 ). The abandonment of the traditional erroneous concept that a pressure dressing is necessary for hemostasis or for healing of the postsurgical neck has almost completely eliminated skin vascular problems including sloughs behind the ears. Excision of skin of the face as well as the neck, and also in the occipital area, requires a closure with less than no tension. The author usually describes the edges as “kissing” when finished except for perhaps 3 small points. In many patients the neck cannot be improved without lifting the face because the facial deep tissues have fallen into the neck. These patients can have support of the superficial musculoaponeurotic system (SMAS) holding up the weight of the skin, which eliminates skin tension in the temporal area as well as the preauricular areas. The positioning of the patient so that the chin-neck angle is at 90° when the occipital skin is excised means that the scar will have less tension. If the patient’s chin is elevated when the skin is excised, the resulting tension when the patient looks downward will create a large scar in the occipital area. Another error frequently seen for both non-Caucasians and Caucasians is the excision of skin in a direction perpendicular to the long axis of the sternocleidomastoid. Even in a 90-year-old patient there is no excessive skin in this direction when the head is moved from side to side.
It is essential to make elevation and separation of the skin from the SMAS and platysma muscle with gentle handling of the tissues. This action permits deep layer support with good skin flap subdermal vascularity. Protection of arterial and venous drainage for the elevated skin flaps permits minimal swelling and discoloration. Postoperative tissue swelling would interfere with the skin blood supply and lymphatic drainage, and should be prevented by precise and near atraumatic surgical technique. Precise elevation of skin flaps with little trauma is made easier by using transillumination. Skin flap trauma with resultant histamine release can be caused by prolonged excessive retraction or forceful scissor shoving, which releases much histamine. Avoiding histamine release and postoperative swelling permits the possibility of safer facelifts for smokers, diabetics, and older individuals.
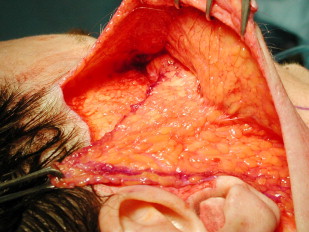
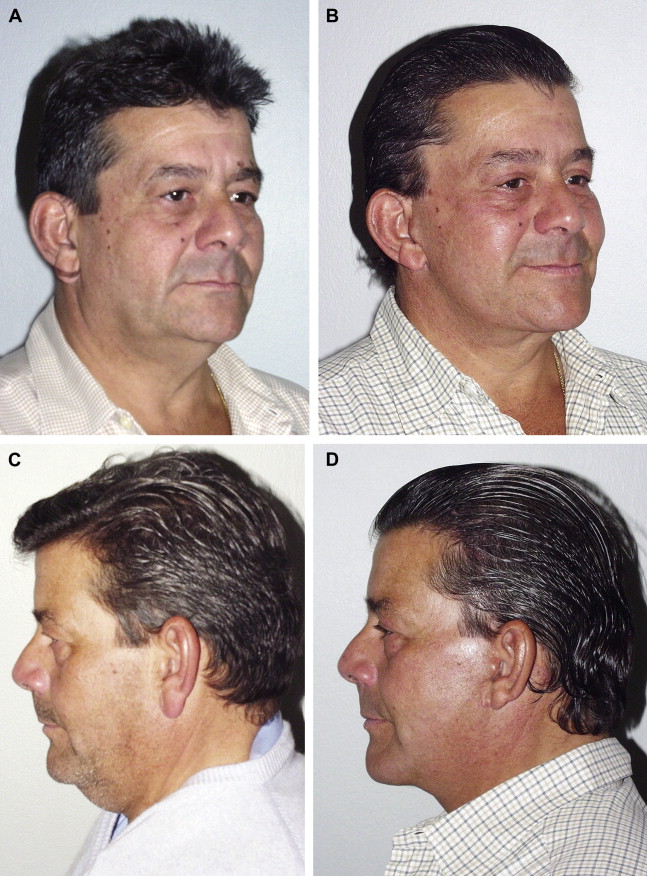
Separation of the skin from the SMAS carries the advantage that the skin and SMAS can be moved along separate vectors and under different tension. This skin-SMAS separation produces a better rejuvenation and a natural appearance. Different vectors of tissue shifting for skin and deep layer support require a high degree of surgical skill to elevate the flaps without thinning the SMAS flap. Unfortunately, use of the SMAS for rejuvenation is not an easy surgical technique. Skill in precise separation of the overlying tissues from the SMAS is essential. This dissection must neither thin the SMAS nor injure the subdermal plexus of arteries and veins. The SMAS is always thick enough to hold sutures unless the dissection technique thins or removes some of the SMAS while elevating the skin flap ( Fig. 3 ). If during the surgical dissection the ability to recognize the SMAS layer and precisely to uncover the intact SMAS is lacking, other less efficient techniques for deep layer support must be used. For most patients, a satisfactory facelift result requires modification of the deep layer support of the SMAS, fascia, and platysma ( Fig. 4 ). When used appropriately, the SMAS will move cheek fat into the eyelid-cheek depression, changing the direction of the nasojugal groove from the diagonal position of old age to the horizontal position of youth, while the malar rotation point provides more malar prominence ( Fig. 5 ).


For non-Caucasian facelift procedures relying on tightening of aging skin flaps in an attempt to elevate and support sagging, deep tissues often have early recurrence of the original deformities. Skin tension results in wide and visible scars. Skin is elastic, and when pressure or weight is applied the skin will stretch. Skin will not support fat and muscles except for a short period of time. The inelastic SMAS can provide sustained support of the deep tissues. To minimize visible scars, redundant skin is excised and the skin closure is made under less than normal skin tension. The difference in tension is noted when the patient is looking downward, looking upward, or turning the head. The restoration of youthful contours is created by restoring the SMAS and attached muscles as well as the facial fat to the same youthful position, and permits a rejuvenated appearance without a tight or postsurgical appearance.
Superficial musculoaponeurotic system
A primary facelift patient always has been found to have a SMAS strong enough to give excellent support to the submental area, depressed angles of the mouth, nasolabial folds, nasolabial grooves, and midface if a high SMAS transection is made. In addition, the high SMAS transection and freeing the smile creases (crow’s feet) reduces excessive skin of the lower eyelid, and can change the diagonal direction of the nasojugal groove from the countenance of old age to the transverse direction of youth. Shortening the lower eyelid can be accomplished only if the smile crease attachments from the skin to the orbicularis oculi muscle are released. The lateral component of the orbicularis oculi, which pulls the lateral eyebrow downward forcefully when smiling, is released by careful transection of only the portion of the muscle acting as a depressor of the orbicularis oculi muscle (depressor orbicularis lateralis). When this transection is made, a muscle flap of orbicularis can add additional support to the lower eyelid by advancing the lower cut edge in a superolateral direction and suturing it to the periosteum. The midface elevation and the sling effect on the submental area by a shift of the SMAS produces excellent submental contour improvement and support (see Fig. 4 ). The midface support by the SMAS results in little or almost no postoperative swelling. There is no risk of lower eyelid ectropion as seen in other mid-facelift surgical techniques (see Fig. 3 ). To make the neck appear youthful, different types of aesthetic neck deformities must be analyzed and precisely diagnosed. An attractive and pleasing appearance requires a well-contoured neck. The neck can indicate age, health, disease, fitness, obesity, beauty, elegance, masculinity, femininity, vitality, strength, and sensuality.
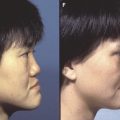
Liposuction and tightening of neck skin is not enough to achieve maximum restoration. Skin tightening will not overcome problems in the deep layer. Rejuvenation by using deep layer facelift techniques includes support with transection of the SMAS at the top or above the zygomatic arch. Often, platysma muscle contour correction and support is needed. The neck lift component of a facelift includes correction of excessive skin, platysma muscle laxity, short platysma muscle, subcutaneous or subplatysmal fat, the anterior belly of the digastric muscle hypertrophy, and large submandibular glands. Tightening of skin over these problems does not correct them. A contour problem frequently not diagnosed is the double chin caused by large anterior bellies of the digastric muscles ( Fig. 6 ). For younger patients who have no sagging subcutaneous tissues and skin of the face, a submental incision alone for digastric muscle reduction is adequate. Submental double chin correction for many patients includes the following components:
- 1.
Tangential removal of 95% of the anterior belly is accomplished by passing a curved hemostat beneath the portion of the muscle to be excised.
- 2.
The muscle is then transected with needle cautery at the insertion at the chin and reflected.
- 3.
The muscle is separated near the sling with a needle coagulating current.
Related posts:
 Hair Restoration in the Ethnic Patient and Review of Hair Transplant Fundamentals
Hair Restoration in the Ethnic Patient and Review of Hair Transplant Fundamentals
 Midface Alloplastic Augmentation in the Asian and Latino Patient
Midface Alloplastic Augmentation in the Asian and Latino Patient
 Middle Eastern Rhinoplasty
Middle Eastern Rhinoplasty
 Lower Facial Rejuvenation in the Non-Caucasian Face
Laser Treatment for Ethnic Skin
Rhinoplasty in the Patient of African Descent
Lower Facial Rejuvenation in the Non-Caucasian Face
Laser Treatment for Ethnic Skin
Rhinoplasty in the Patient of African Descent
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


