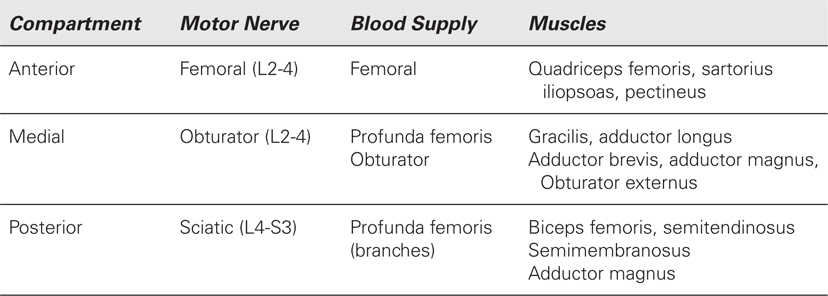
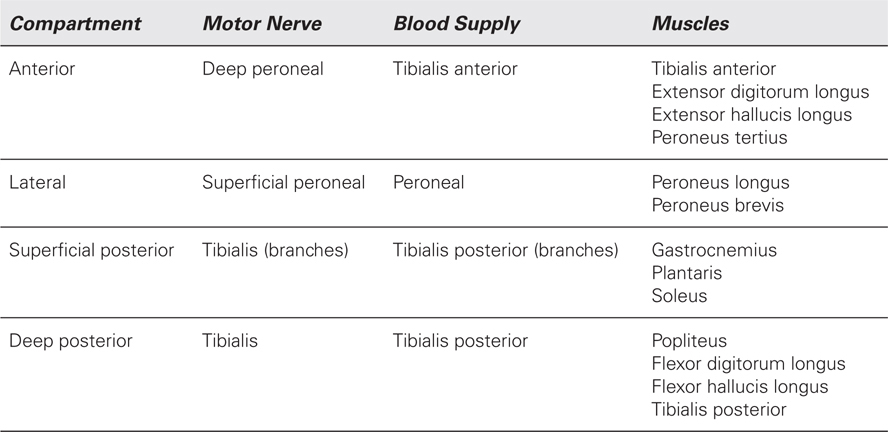
How many compartments exist in the thigh and leg? Which muscles, nerves, and blood vessels lie in which compartments?
Thigh (Table 87-1)
Lower Leg (Table 87-2)
 Which nerves supply sensation to the foot?
Which nerves supply sensation to the foot?
• Dorsum: superficial peroneal except the first web which is supplied by the deep peroneal.
• Sole: medial and lateral plantar from the posterior tibial.
 What are the biomechanical effects of the foot that make reconstruction potentially suboptimal?
What are the biomechanical effects of the foot that make reconstruction potentially suboptimal?
Normal gait requires the foot to transition from a flexible structure to a rigid structure as the hindfoot makes contact and forces are transitioned to the forefoot. The forefoot’s unique osteoligamentous structures facilitate this conservation of energy. Current flap techniques cannot replicate the biomechanics of the intact foot.
 What percentage of patients with diabetes mellitus develops heel ulcers?
What percentage of patients with diabetes mellitus develops heel ulcers?
15%.
 What are the possible biomechanical effects on the foot of patients with diabetes mellitus?
What are the possible biomechanical effects on the foot of patients with diabetes mellitus?
• Reduced subtalar joint mobility.
• Limited first metatarsal mobility.
 What is a Charcot foot?
What is a Charcot foot?
It is acute or gradual arthropathy of the foot that most commonly occurs in patients with diabetes. It was originally described in patients with syphilis. The pathophysiology of the disease has not been definitively elucidated but it may involve trivial microtrauma that affects the joints of the foot. Another theory attributes autonomic changes that lead to increased osteopenia of the bones. Swelling, erythema, pain, and ulceration (40%) may develop that mimics infection. Collapse of the osseoligamentous structures of the foot leads to derangements in pressure points on the foot.
 What is the most common location of bony sarcomas of the lower extremity?
What is the most common location of bony sarcomas of the lower extremity?
Proximal tibia.
 What are the most common complications of limb salvage for these sarcomas?
What are the most common complications of limb salvage for these sarcomas?
• Wound healing (skin flap necrosis).
• Wound infection.
• Nerve palsy.
• Hardware failure.
 What are the treatment options of resectable bony sarcomas of the distal femur and proximal tibia?
What are the treatment options of resectable bony sarcomas of the distal femur and proximal tibia?
• Amputation.
• Reconstruction with oncologic appliance and soft-tissue flap.
• Rotationplasty (children).
 Why is it necessary to perform flap coverage of the knee oncologic appliance for tumors of the distal femur/proximal tibia?
Why is it necessary to perform flap coverage of the knee oncologic appliance for tumors of the distal femur/proximal tibia?
Wound complication rates of over 50% have been reported with prosthesis placement without flap coverage. Malignant lesions in this region require resection of adjacent soft tissue, skeletonization of neurovascular structures, and development of large subcutaneous flaps. This leads to an increased risk of implant exposure and infection without the use of adjunctive flap coverage.
 What is a Girdlestone procedure?
What is a Girdlestone procedure?
Described in the 1940s, it is resection of the femoral head and neck for severe infection of the hip. Although the procedure is uncommon in the modern era, it is still employed for severe stage IV trochanteric pressure ulcers complicated by osteomyelitis. The vastus lateralis muscle flap may be employed to interpose in the dead space created by the resection.
 What are the ambulatory implications of a Girdlestone procedure?
What are the ambulatory implications of a Girdlestone procedure?
The leg will be shorter and require the patient to be dependent on walking aids, such as a walker or crutch.
 What are the possible clinical circumstances of a peroneal nerve injury?
What are the possible clinical circumstances of a peroneal nerve injury?
• Fracture of a tibia or fibula.
• Sharp injury.
• Severe adduction injury of the knee.
• Gunshot wound.
• Iatrogenic (ganglion resection, fibula harvest).
 Why should tourniquet placement directly below the knee (proximal leg) be avoided?
Why should tourniquet placement directly below the knee (proximal leg) be avoided?
Peroneal nerve palsy with compression at the head of the fibula may develop. Place the tourniquet above the knee. Avoid tourniquets in patients with vascular bypass grafts across the region of tourniquet control.
 If the common peroneal nerve is disrupted, what are the treatment options?
If the common peroneal nerve is disrupted, what are the treatment options?
• Primary repair of nerve in the low-energy or sharp injury with or without nerve graft. This can be performed immediately or within weeks after the injury.
• Tibialis posterior transfer. Since an equinovarus deformity inevitably develops despite use of a kick-up brace, muscle balancing with early tendon transfer may be advantageous.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


