Evolution in extremity injury treatment often occurs during major conflicts, with lessons learned applied and translated among military and civilian settings. In recent periods of war, improvements in protective equipment, in-theater damage control resuscitation/surgery, delivery of antibiotics locally/systemically, and rapid evacuation to higher levels of medical care capabilities have greatly improved combat casualty survivability rates. Additionally, widespread application of lower extremity tourniquets also has prevented casualties from exsanguination, thus reducing hemorrhagic-related deaths. Secondary to these, a high number of combat casualties suffering lower extremity traumatic injuries have presented for functional limb reconstruction and restoration as well as residual limb care.
Key points
- •
Lessons learned in extremity restoration and residual limb care secondary to combat trauma rapidly transfer among military and civilian centers as well as vice versa.
- •
Experience of surgical and medical teams treating extremity injuries has a direct impact on decision making and algorithm adoption, which have a positive impact on treatment measures and outcomes.
- •
Microsurgical techniques and advancements in orthoplastic surgery, including perforator and chimeric flaps; peripheral nerve surgery, including repair strategies and nerve transfer applications; and bone as well as soft tissue regeneration techniques and regenerative medicine increasingly have been applied to restoration of war-related traumatic lower extremity injuries.
- •
Functional limb restoration and residual limb patients require rehabilitation and potential ongoing surgical care measures that can span their lifetimes after initial traumatic injury recovery.
- •
An integrative, collaborative multidisciplinary team approach to extremity injury treatment and ongoing care needs is a desired state and ultimate goal.
Background
Plastic surgery has a long history of innovation when faced with wartime challenges. Most surgeons attribute the birthplace of modern plastic surgery to the European trenches of World War I. The protection of vital structures and relative exposure of the face saw the return of many soldiers with devastating facial injury. These challenges allowed Morestin, Valadier, and later Gilles to establish new techniques to reconstruct the maxillofacial injuries. In World War II, the advent of militarized aviation led to a greater proportion of shrapnel injuries and fuel tank explosions. Sir Archibald McIndoe pioneered modern burn care and used many of the techniques described by Gilles to reconstruct his badly disfigured patients. These men who were willing to undergo cutting edge procedures for a chance at rehabilitation self-named themselves, “The Guinea Pig Club.” During the same period, Dr Sterling Bunnell’s contributions, as a consultant to the US Army, directly increased the understanding and treatment of hand injuries in which time he personally treated more than 20,000 combat-related hand injuries. His efforts led to the definitive textbook and background for all hand surgery training programs for decades and beyond.
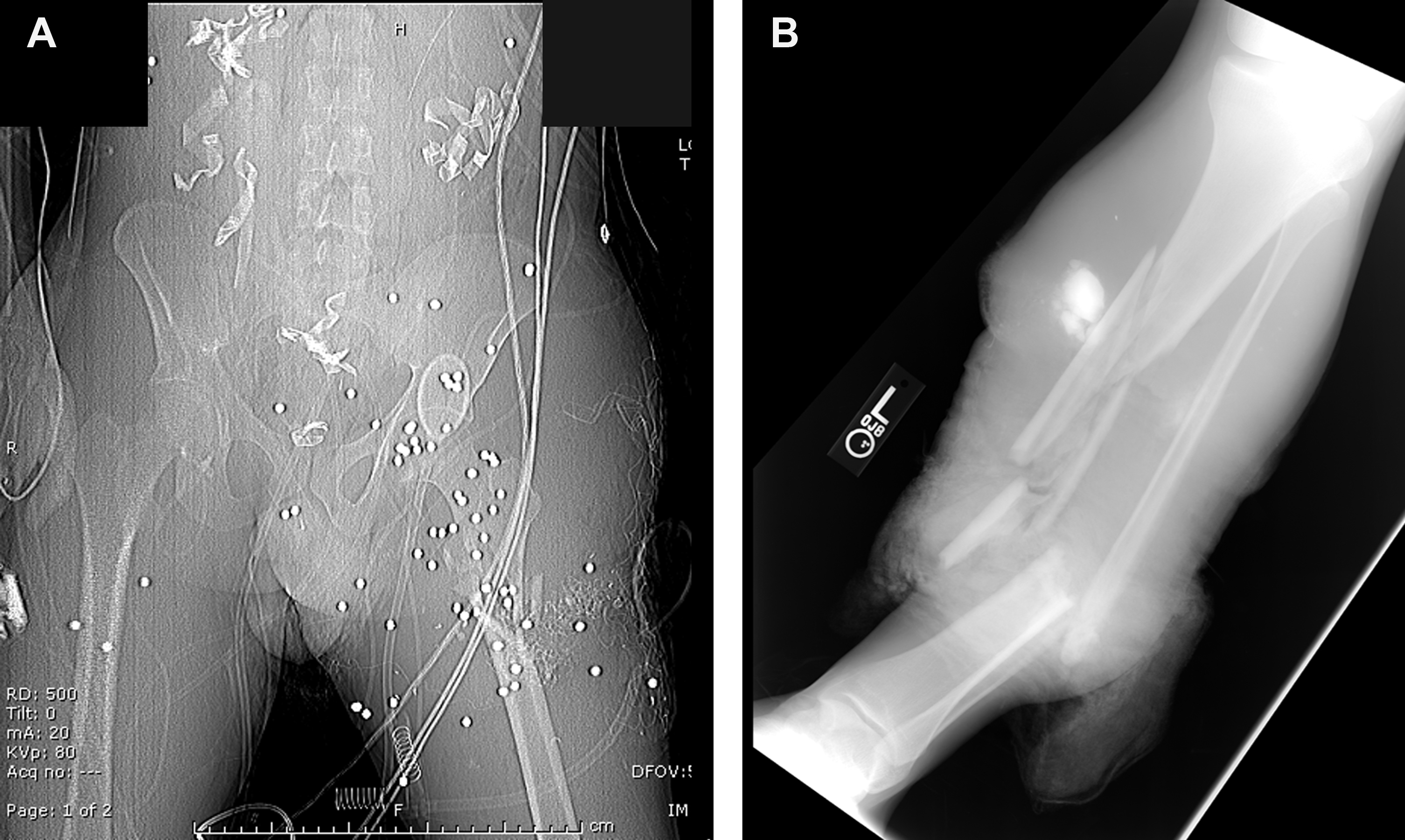
Modern conflict presents extremity reconstructive surgeons with a new set of challenges when treating combat casualties returning from the war theater. The recent conflicts in Iraq and Afghanistan now represent the longest sustained engagement in American military history. Analysis of the injuries incurred by American combat casualties reveal a marked increase in the proportion of complex extremity injury compared with injuries of the same type sustained in previous wars. , This observation within the US military medical care setting was paralleled by a comparative British study, which also reported approximately half of all injuries to trauma patients were to the extremity, with the largest proportion affecting the knee and/or lower leg. This shift in injury patterns can be attributed to several factors. First, modern warfare has brought about the widespread use of individual protective body armor and Kevlar (DuPont, Wilmington, DE) helmets. These protective measures have greatly reduced life-threatening thoracic and head injury, yet, in turn, created an increase in extremity injury following combat-related trauma. Additionally, the higher rates of indirect ambush attacks and utilization of improvised explosive devices (IEDs) by enemy combative forces and terrorists have increased the proportion of ballistic injuries incurred to the lower extremities. These weapons and associated high-energy blasts often result in composite tissue defects consisting of open fracture(s) with variable comminution patterns, severe soft tissue losses, and potential concomitant thermal injury as well as high rates of contamination with various particulates and foreign debris ( Fig. 1 ). Given the threat of exsanguination from extremity injuries suffered during combat, algorithms have been implemented for the improved use of tourniquet application, leading to a tremendous reduction in hemorrhagic deaths while further increasing the number of combat casualties requiring extremity reconstruction and restoration measures. ,
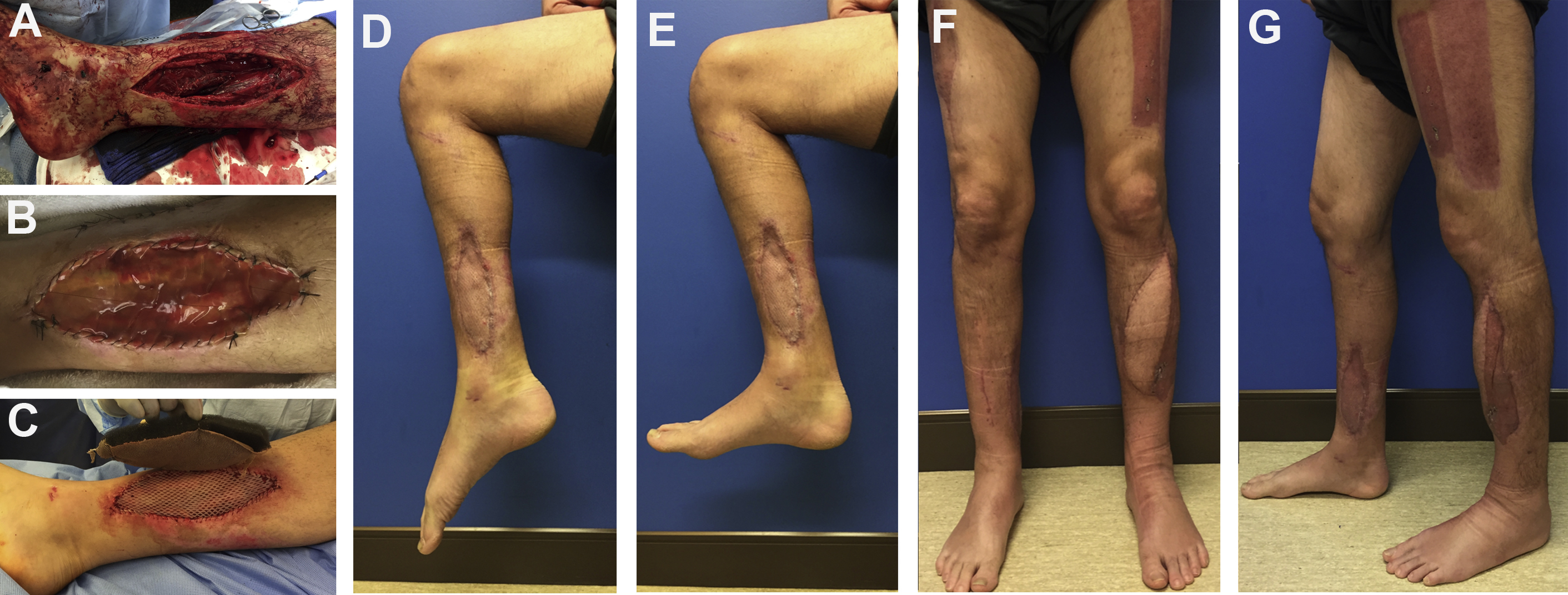
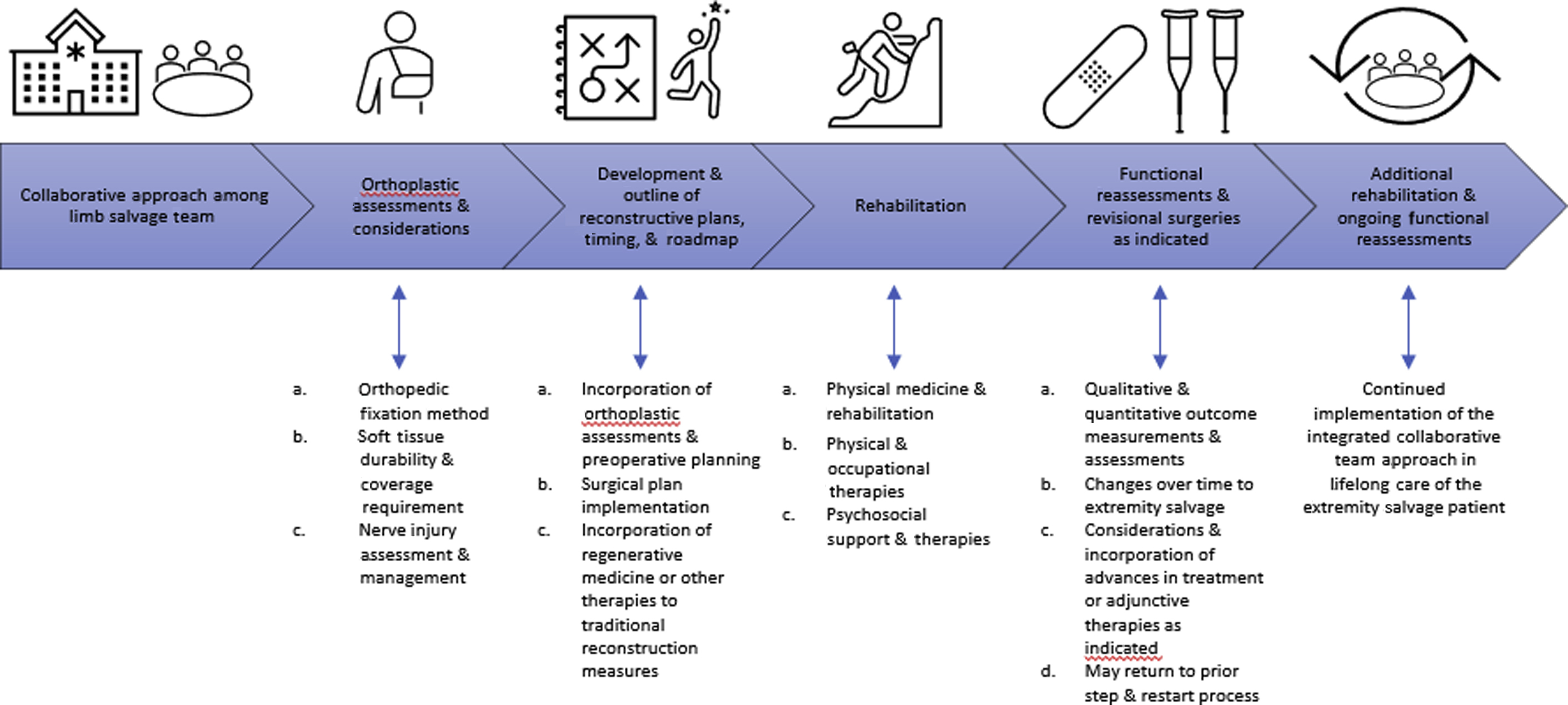
Reconstructive surgeons have advanced beyond the more simplistic concept of “limb salvage” to that of “functional limb restoration” ( Figs. 2 and 3 ). The goal of limb salvage is to recover the form and function of the lower extremity to the greatest extent possible. A salvaged limb that has ongoing neuropathic pain and/or significant functional deficits, however, is not nor should no longer be considered a success. Therefore, the primary idealized goal of extremity reconstruction is to restore the function and stability of the injured lower extremity while minimizing neuropathic pain and related disabilities—that is, functional limb restoration. This article highlights the lessons learned; outlines various principles, concepts, and best-known practices; and reflects on techniques that aid in functional limb restoration from lower extremity injuries suffered by wounded warriors. How an integrated, collaborative care model ( Fig. 4 ) for ongoing lifelong care either for limb restoration or residual limb patients is the desired state to optimize the care of those patients suffering from severe lower extremity injury(-ies) also is presented.

Initial considerations and triaging lower extremity injuries on the battlefield
Regardless of whether an injury occurs on the battlefield or in civilian life, severe extremity trauma first should be managed by life-saving measures, including stopping the bleed or rapid tourniquet application, followed by assessment and establishment of supportive airway and breathing measures (circulation, airway, and breathing). A primary survey should be conducted expeditiously to identify any active hemorrhage that can be controlled by direct pressure or tourniquet application. Consideration for primary amputation should be made only in instances where there are no options for limb preservation that would convey some return to function or form of the affected limb. Reports have shown that there are few indications for primary amputation if limb preservation is not a threat to a patient’s life. Limb preservation at index operations may allow time for emotional acceptance of eventual amputation and has been shown to be cost effective in at least 1 study.
Once the patient is stabilized, a thorough secondary survey, including comprehensive physical lower extremity examination, should document any soft tissue losses, identify any non–life-threatening vascular injury(-ies), associated nerve injury(-ies), muscle-tendon deficits, and concomitant bony injury(-ies). Initial radiographs to determine the extent of bony injury using a portable radiograph once in the military trauma bay because orthopedic injury should heighten the suspicion for neurovascular injury. These studies should not interfere, however, with a more diagnostic computed tomography (CT) with or without angiography scan when indicated. These studies can provide more robust examination of soft tissue defects and vascular integrity when combined with a lower extremity angiogram.
Damage control and management of lower extremity wounds
Once life-threatening injuries are stabilized, the orthoplastic surgical management of a mangled or severely injured lower extremity can be broken down into the treatment of the associated bone, neurovascular, and soft tissue injuries. Consideration of the orthopedic fixation method, nerve injury assessment and management, and soft tissue coverage for durability and tolerance of potential revisional surgeries to be collectively employed should be outlined and mapped among the integrated team. Unstable fractures and joints should be stabilized initially with in-line traction, Kirschner wires, external fixators, or plaster splints prior to eventual definitive fixation (see Fig. 2 ). Soft tissue injuries must undergo early, aggressive, and serial débridement as well as irrigation of all nonviable skin, muscle, and other soft tissues of the lower extremity, typically every 2 days to 3 days. These measures rid the wound of nonviable tissues, which are a nidus for infection, while subsequently diluting any contaminants to the wound bed of the extremity. Most ballistic and high-energy trauma patients should be treated initially with broad-spectrum antibiotic therapy. In general, a short course using broad-spectrum antibiotics is recommended in any open fracture trauma, but coverage should be tailored to the nature of the injury and the microbiome of the environment in which the injury occurred. There have been reports of reduced risk of infection of traumatic lower extremity wounds when using antibiotic-impregnated polymethyl methacrylate beads to deliver a concentrated source of antibiosis at the site of injury, while various orthoplastic surgeons have utilized absorbable antibiotic beads to aid in local infection reduction control measures. Several publications support the use of negative-pressure wound therapy with or without incorporation of irrigation solutions (eg, instillation of saline or topical irrigant solutions), such as Dakin solution (sodium hypochlorite) or Vashe solution (hypochlorous acid), when awaiting time to definitive orthoplastic reconstruction and soft tissue coverage.
Lower extremity vascular injury
The initial assessment for vascular injury should include examination of hard signs, including active hemorrhage; large, expanding, or pulsatile hematoma; bruit or thrill over the wound; absent distal pulses; and any distal ischemic manifestations, such as pallor, paresthesia, or poikilothermia. Kelly and colleagues suggested that physical examination alone has sensitivity to rule out ischemic injury. Once vascular injury is suspected, prompt CT angiography is paramount for diagnosing the level of injury and allows for more precise surgical planning prior to the operating room. If perfusion must be restored but definite vascular repair either is not advisable due to patient condition or infrastructure capabilities, the use of temporary shunting has been championed. , Rasmussen and colleagues used data analysis of combat casualties suffering extremity injuries with vascular compromise in Iraq to conclude that the use of shunts was an effective stopgap to temporize perfusion during immediate evacuation rather than attempt reconstruction in remote locations. These findings have been extrapolated to civilian trauma centers where temporary shunting has been employed for certain extremity trauma.
In scenarios where shunting is not feasible, the redundant nature of the lower leg circulation allows for ligation of 1 of the 3 dominant vessels (anterior tibial, posterior tibial, and peroneal) without compromising the perfusion to the foot. Burkhardt and colleagues suggested that revascularization can be deferred if 1 tibial vessel remains patent if the foot is warm and well appearing on clinical examination. If both anterior and posterior tibial arteries are injured, distal bypass often is required. Perfusion via only the peroneal artery typically is inadequate for foot salvage. Outside of distal bypass procedures, the authors’ group also has utilized flow-through flap options for concurrent soft tissue coverage and reconstitution of arterial and venous outflow in severe combat-related dysvascular lower extremity injuries. Ligation of larger and more proximal vessels at the level of the thigh can be more perilous. Arterial ligation at this level is more likely to lead to distal ischemia and should be monitored closely postoperatively. Venous ligation often leads to acute hypertension due to inadequate outflow. Ideally, vascular repair should occur within 6 hours from injury because there is evidence that ischemia time longer than 6 hours portends increased risk of amputation. The most common flaps employed as flow-through flaps consisted of the anterolateral thigh flap with and without inclusion of the vastus lateralis muscle utilizing the descending branch of the lateral circumflex vessels, the omentum and its gastroepiploic vessels; the rectus abdominis and perforator flap variants (muscle-sparing free transverse or vertical rectus abdominis and/or the deep inferior epigastric perforator flaps) based on the deep inferior epigastric vessels, the subscapular based vessels supplying the latissimus, thoracodorsal artery perforator; scapular and parascapular flaps, as well as the osseous-, osteocutaneous, and osteomyocutaneous flaps utilizing the fibula and its parent peroneal vessel system.
Postoperative monitoring of vascular repair should include baseline graft duplex studies or ankle-brachial index values to assess efficacy of revascularization. Routine duplex study often is regarded as the best noninvasive method for surveillance of repair patency. Careful clinical monitoring via physical examination of distal perfusion may be as effective as intensive. The intermediate postoperative period (3–18 months) often is the time where a significant number of repairs fail. Failure in this time period most often is a result of myointimal hyperplasia with vein grafts. Late failure often is a result of naturally progressive atherosclerosis.
Lower extremity nerve injury
Peripheral nerve injuries that are incurred following a combat injury represent a complex surgical problem. The mechanism of injury from penetrative or ballistic force often results in severe orthoplastic injury that can cause transection, stretch, or shear injuries on nearby peripheral nerves. Although damage to upper extremity nerves can have more deleterious effects on function given their relationship to the hand, major peripheral nerves in the lower extremity were also associated with poor outcome, historically. , A thorough clinical examination along with electrodiagnostic testing accompanied by magnetic resonance imaging (MRI) can inform the surgeon regarding the extent of the peripheral nerve injury. There also is utility in high-definition ultrasound as a diagnostic tool, particularly when metal fragments are retained or anatomy is grossly distorted, thus limiting the reliability of MRI or electromyographic studies.
Once peripheral nerve injuries are identified and documented, established and newly founded indications for repair increasingly have been pursued in combat casualty extremity trauma in an effort to reduce functional deficits and neuropathic pain development. Cleanly transected nerves, although less common in war-related extremity trauma, can be repaired primarily with end-to-end suture techniques if the resultant repair does not result in unfavorable tension after neurolysis and preparation of the nerve. One of the key principles employed is sharp débridement of the peripheral nerve to healthy fascicles when possible to permit better nerve regeneration and repair. If a tension-free coaptation cannot be achieved after debridement and preparation of the nerve, reconstructive surgeons can employ several adjunctive techniques to aid in peripheral nerve repair. Specifically, small gaps less than 1 cm can be repaired with nerve conduit to aid in achieving a tension-free repair. Larger gaps exceeding 1 cm in length often require either nerve autograft or processed cadaveric nerve allograft for reconstruction of the nerve. In general, selection of appropriate donor nerves for autograft or allograft should consider the size of segmental gap encountered, the proximity to recipient nerve motor end plates or distal target end organ for reinnervation, redundancy of donor nerves, synergism of donor muscles to target muscles, and size matching for effective nerve repair and regeneration.
In combat casualties suffering complex injury patterns, a subacute repair can at times be advantageous. In these situations, the extent of nerve injury often does not present itself until edema resolution and resulting scar formation occur. In these cases, nerve ends often are marked during initial exploration with spanning Prolene (Ethicon, Cincinnati, OH) or nylon sutures for delayed repair procedures. Definitive reconstruction ideally is performed within 3 weeks to 6 weeks of the initial injury. This delay also may have the added benefit of allowing for adequate débridement, treatment of concomitant injury, declaration of soft tissues, and control of infection in the affected extremity. Delay should not exceed 3 months following injury because Jonsson and colleagues reported that this may represent a critical time point after which repair strategies have significantly worse outcomes, and delay in repair can lead to less optimal outcomes, especially regarding critical motor end plate reinnervation.
Residual paralysis from nerve injury that does not achieve meaningful functional recovery via nerve repair can be treated with tendon transfers, nerve transfers, and/or neurotized flap reconstruction in certain cases. In the lower extremity, the most effective reconstructive method to preserve stability and prevent foot deformity in peroneal nerve palsy continues to be tibial tendon transfer (tibialis posterior to tibialis anterior) or the Ninkovic procedure (lateral gastrocnemius muscle and tendon transfer with neurotization via transfer of the peroneal nerve to the lateral sural nerve to the lateral gastrocnemius muscle). ,
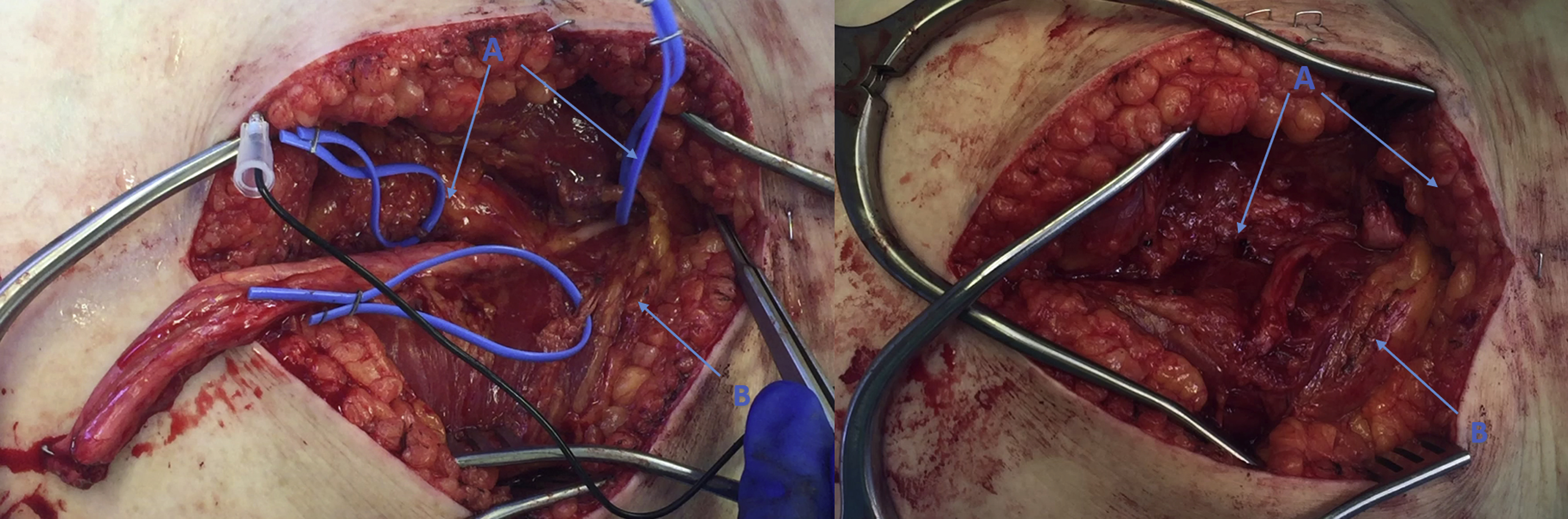
Apart from motor nerve injury, damage to sensory nerves can result in neuropathic pain that mirrors phantom limb pain (PLP) or the perception of discomfort in a limb that is no longer present as seen in residual limb patients. This poorly understood phenomenon can occur in up to 85% of patients with traumatic loss of limb and can be experienced in patients suffering major peripheral nerve injury to their salvaged limb. In addition, the formation of symptomatic neuroma at peripheral nerve blind endings can result in neuropathic pain further irritated by pressure, light touch, and even temperature variation. Knowing this, targeted muscle reinnervation (TMR) or regenerative peripheral nerve interface (RPNI) often are employed as measures to mitigate the formation of neuroma and prevent neuropathic pain in not only residual limb patients but also patients undergoing functional limb restoration in cases where nerve reconstruction cannot be had (eg, large segmental nerve injuries where autografting or allografting is not likely to contribute to complete functional nerve recovery) ( Figs. 5–8 ). Using these techniques, peripheral nerve endings without end-organ targets are transferred to recipient motor nerves and freshly denervated motor end plates of residual muscle or to free muscle grafts to allow for more organized neurite outgrowth and reinnervation of the target muscle and muscle grafts. Armed with the promise of these initial results, reconstructive surgeons often now apply these techniques in a prophylactic manner for lower extremity patients with traumatic nerve injuries, which in turn has shown to have a significant effect in the prevention of neuroma and PLP (see Figs. 7 and 8 ). This preemptive approach to treating PLP and symptomatic neuroma has been shown to decrease pain severity in patients following traumatic amputation and in limb restoration patients.
Related posts:
 Propeller Flaps in Lower Extremity Reconstruction
Propeller Flaps in Lower Extremity Reconstruction
 The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
 Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
 Microsurgical Reconstruction of the Lower Extremity in the Elderly
Microsurgical Reconstruction of the Lower Extremity in the Elderly
 Orthoplastic Approach to Lower Extremity Reconstruction
Orthoplastic Approach to Lower Extremity Reconstruction
 Lower Extremity Reconstruction in the Pediatric Population
Lower Extremity Reconstruction in the Pediatric Population
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


