Surgical resection with wide margins and perioperative radiation therapy is the standard treatment of extremity soft tissue sarcomas. This combination often results in complex wounds and functional compromise. Reconstructive surgery is integral to limb salvage after sarcoma resection. Advances in adjuvant therapy and reconstructive surgical techniques have made functional limb salvage, instead of amputation, possible for most patients. This article reviews key concepts in the multidisciplinary care of patients with extremity soft tissue sarcomas and details reconstructive surgical techniques, including locoregional and free tissue transfer, free functional muscle transfer, and vascularized bone transfer, to optimize functional limb restoration after sarcoma resection.
Key points
- •
Localized extremity soft tissue sarcomas (ESTS) frequently arise in the lower extremity and account for 1% of all adult tumors.
- •
Oncological treatment of ESTS involves wide surgical resection, often combined with perioperative radiation therapy. After tumor resection, many patients will have complex soft tissue defects that require reconstructive surgery to achieve functional limb restoration.
- •
The role of amputation in the treatment of ESTS has steadily declined. Advancements in adjuvant therapy and reconstructive surgical techniques, including microsurgical free-tissue transfer, functional muscle transfer, and vascularized bone transfer, have made functional limb salvage attainable in greater than 90% of patients.
- •
A multidisciplinary team of oncological surgeons, radiation oncologists, medical oncologists, plastic surgeons, and physical therapists is essential to optimizing oncological and functional outcomes in patients with ESTS.
Introduction
Soft tissue sarcomas (STS) are a heterogenous group of tumors with mesenchymal origin that account for 1% of all cancers. Anatomically, greater than 30% of STS arise in the lower extremities. Surgical resection with wide margins is the primary treatment option for localized extremity soft tissue sarcoma (ESTS). Surgical treatment must balance oncological considerations with functional considerations. Historically, the extent of resection to attain local control resulted in substantial morbidity and, often, amputation. Over the last 40 years, the role of amputation in ESTS has steadily declined due to radiation therapy (RT) and the publication of landmark studies demonstrating no improvement in overall survival (OS) for patients undergoing amputation versus limb-sparing surgery combined with adjuvant therapy. , Today, tumor resection with an emphasis on limb preservation is attainable in greater than 90% of patients with ESTS.
Because limb preservation has become standard, maintaining or restoring functionality of the limb is imperative. Unfortunately, the combination of wide resection and RT in the lower extremity often results in functional compromise and complex wounds. In these scenarios, reconstructive surgery plays an integral role. The goals of reconstructive surgery following surgical resection are functional limb restoration and wound closure that minimizes complications and delays in adjuvant treatment. Inclusion of plastic surgeons improves the rates of limb salvage and enhances functional and aesthetic results following ESTS resection.
In this article, the authors outline important considerations in the multidisciplinary care of patients with ESTS and propose an anatomic and defect-centered approach to lower extremity reconstruction that emphasizes functional limb restoration. In cases where limb preservation is not possible, the authors advocate for amputation with contemporary reconstructive surgical techniques to maximize residual limb function with a prosthesis and minimize neuropathic pain.
Preoperative evaluation: multidisciplinary care, imaging, and staging
Patients should be evaluated in comprehensive cancer centers by a multidisciplinary team, including oncological surgeons, orthopedic surgeons, plastic and reconstructive surgeons, medical oncologists, and radiation oncologists. Patients with ESTS treated at high volume cancer centers have significantly better survival rates and functional outcomes. In addition, this may avert unplanned excisions of ESTS, which are associated with increased rates of local recurrence and can contribute failed limb salvage.
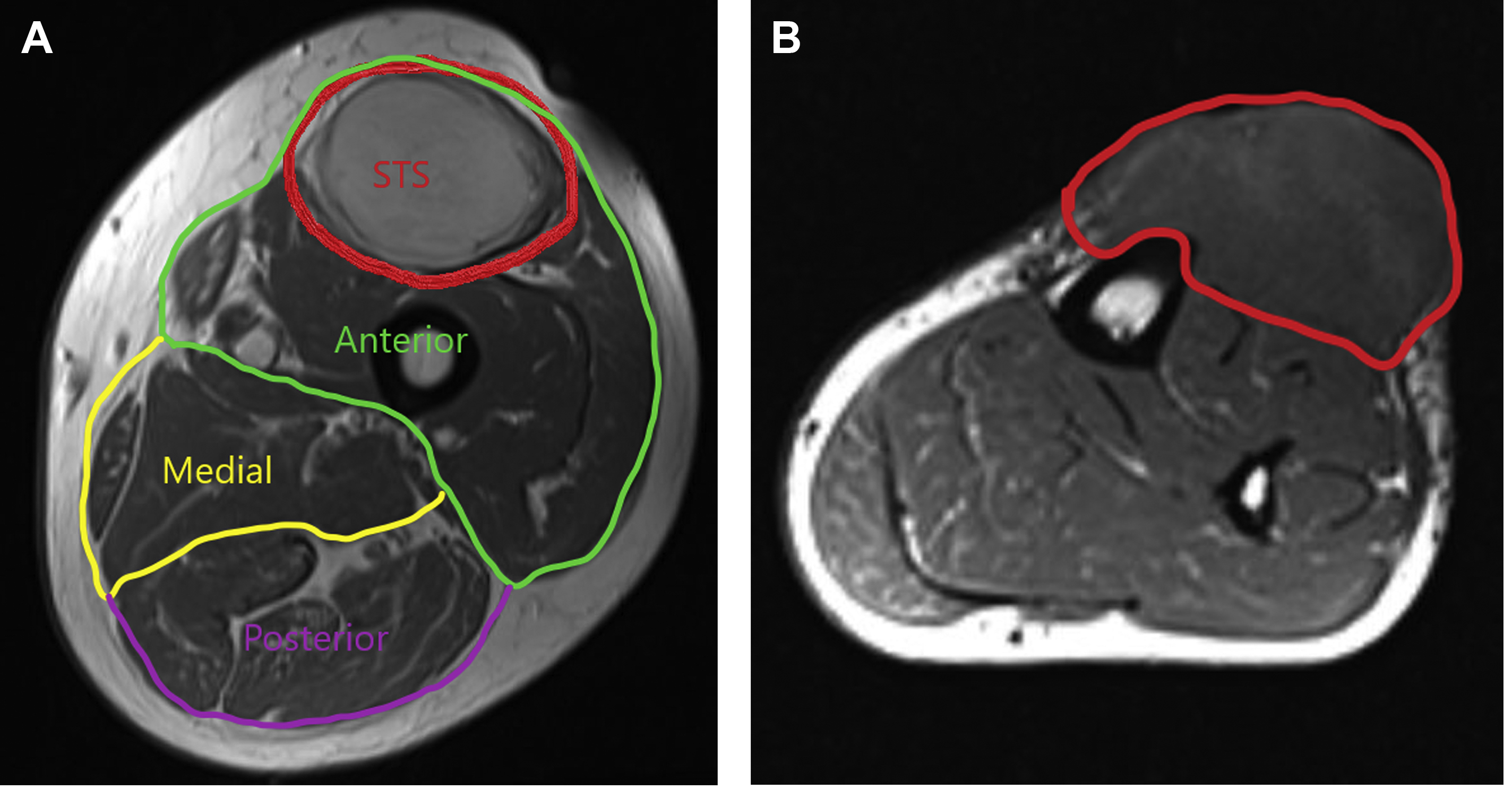
MRI remains the standard for evaluating soft tissue masses. MRI provides detailed visualization of tissue planes and compartments, facilitating staging and surgical planning ( Fig. 1 ). With imaging, the reconstructive surgery team can anticipate the defect and plan accordingly.
Diagnosis of ESTS is confirmed with histologic assessment. Tissue specimens are most frequently obtained with core needle biopsy, but a carefully planned excisional biopsy is also suitable for small tumors. ESTS are staged according to the American Joint Committee on Cancer (AJCC) 8th edition system. Histologic grade, tumor size, and depth are drivers of prognosis in ESTS. Additional adverse prognostic factors are older age, proximal tumor location, and local recurrence.
Oncological treatment: role of surgical resection, radiotherapy, and chemotherapy
The National Comprehensive Cancer Network (NCCN) guidelines recommend wide surgical resection with oncologically appropriate margins for localized ESTS. Resection of the tumor pseudocapsule and a margin without microscopic disease (>1 cm) significantly reduce local recurrence. The NCCN guidelines also support RT and chemotherapy as adjuvant options.
RT can reduce the risk of local recurrence in ESTS with high-risk features (high-grade tumors, large tumors, deep tumors, tumors abutting neurovascular structures, and tumors with select histologic subtypes). , , Preoperative and postoperative RT are demonstrated to facilitate limb preservation. When indicated, our preference is preoperative RT. Preoperative RT involves lower doses and irradiates a smaller tissue volume, resulting in lower rates of fracture, joint stiffness, tissue fibrosis, and functional compromise compared with postoperative RT. A recent study of more than 27,000 patients with ESTS demonstrated preoperative RT independently predicts R0 (margin-free) resections and may improve OS. Furthermore, prior publications have confirmed preoperative RT does not increase wound complications in patients undergoing reconstructive surgery after sarcoma resection and may be associated with fewer complications compared with postoperative RT. In situations where oncologically appropriate margins are not obtained, reresection with negative margins and/or adjuvant RT are indicated.
The role of chemotherapy should be determined on a case-by-case basis. Across the heterogenous group of STS, a meta-analysis of randomized controlled trials revealed chemotherapy has only had marginal efficacy on reducing local recurrence and improving OS. The NCCN guidelines support chemotherapy as a Category 2A recommendation (uniform consensus that the intervention is appropriate based on lower-level evidence). Ultimately, the potential benefits of chemotherapy should be balanced with the associated systemic toxicities.
Limb salvage: indications and contraindications
The decision to proceed with limb salvage is influenced by oncological and functional considerations. Limb preservation with adjuvant therapy is oncologically equivalent to amputation in regard to disease-free survival and OS. Traditionally, if resection involved neurovascular structures or compromised residual limb function, then amputation was performed. In the current paradigm, these factors are no longer contraindications to limb salvage. Preoperative RT can improve local control and reduce the aggressiveness of resection. Even when tumors involve neurovascular structures, studies have demonstrated limb salvage is feasible if these structures can be reconstructed. , Furthermore, if large resections of muscle compartments are necessary for local control, function can be restored with techniques such as functional muscle transfers. With multidisciplinary collaboration and careful planning, functional limb preservation and restoration can be accomplished in most patients.
However, limb salvage is not always warranted. If function is expected to be poor even after reconstructive surgery, then amputation is a better option. Often, this occurs in recurrent tumors that are large, multifocal, or proximally located. Other common indications for amputation are in fungating tumors or when tissue contamination is present. , In patients with metastatic disease and a painful tumor, amputation may provide an equivalent palliative benefit with a shorter recovery period. When amputation is indicated, contemporary reconstructive surgical techniques, as discussed later, should be used to optimize outcomes.
Timing of Reconstruction
Immediate reconstruction has several advantages and is our preferred approach. Foremost, it obviates an open wound that may potentially delay adjuvant therapy. In addition, it facilitates earlier rehabilitation. Surgically, it enables a more straightforward operation, as tissue edema, fibrosis, and scar formation are minimal. Immediate reconstruction is also associated with less morbidity and a lower risk of wound infection and dehiscence compared with delayed reconstruction. The main indication for delayed reconstruction is resection with uncertain margin status. In these cases, the authors advocate for placement of a vacuum-assisted closure device followed by definitive reconstruction when margins are clear.
Reconstructive surgical procedures: anatomic and defect-specific approach
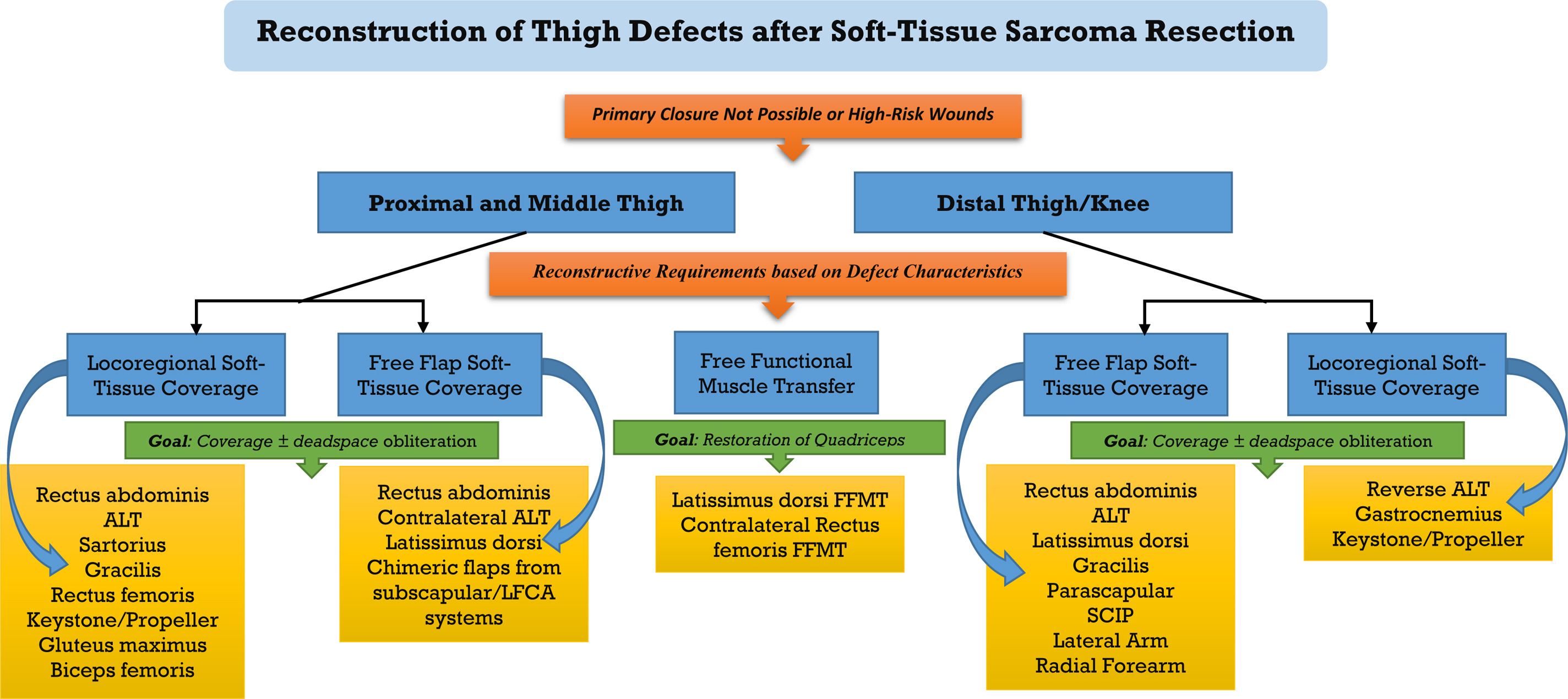
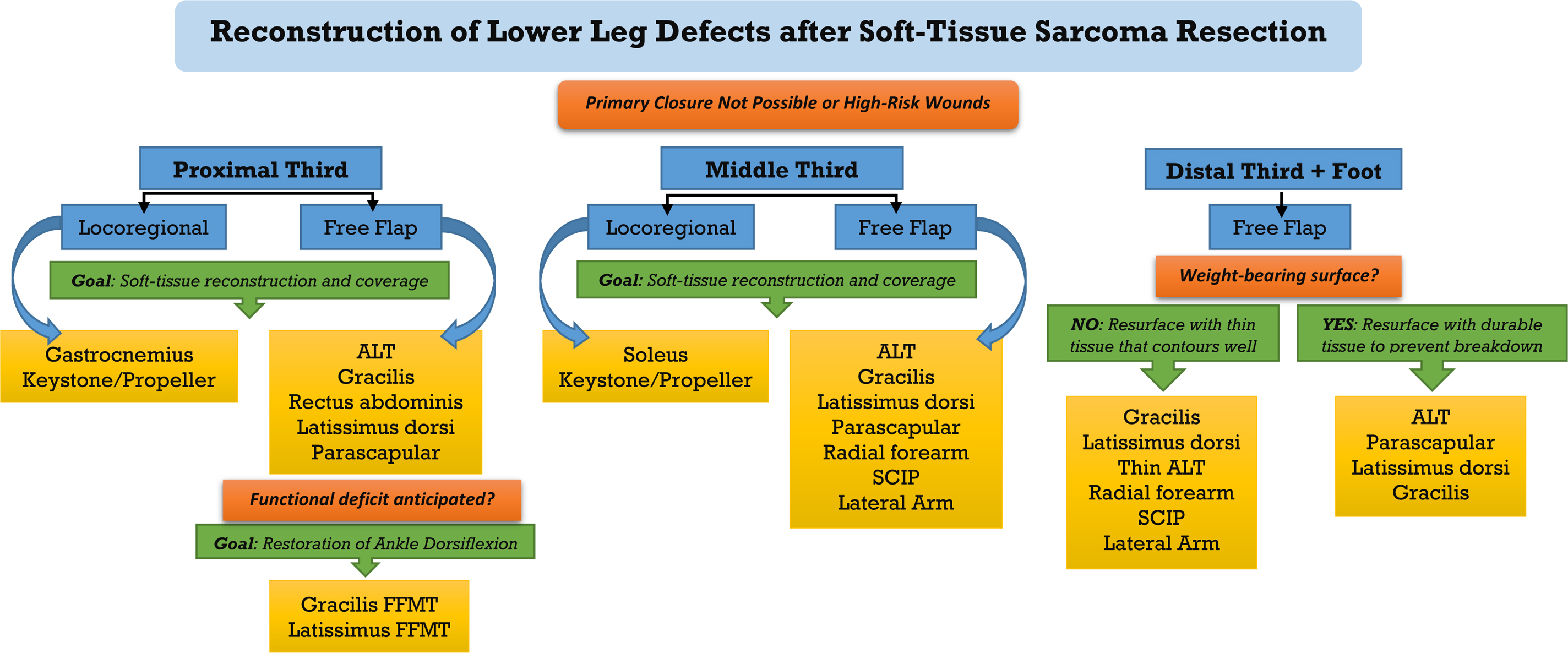
The approach to reconstruction is dictated by defect size, location, expected functional loss, involvement of underlying structures, and receipt of RT. Primary wound closure can be achieved following resection of most small tumors. In wounds with vascular tissue at the base, skin grafting can be attempted; however, in our experience, skin grafting to a radiated field has unfavorable outcomes. Factors known to cause major wound healing complications requiring more involved reconstructive approaches are RT, tobacco use, diabetes, tumor size (>10 cm), proximity to the skin surface (<3 mm), and exposure of major neurovascular structures. , When reconstructive surgery is indicated, we advocate for an anatomic and defect-specific approach that emphasizes functional restoration. We present our algorithm for reconstruction of defects located in the thigh and lower leg in Figs. 2 and 3 , respectively.
Thigh
Proximal and middle thigh
Locoregional soft tissue reconstruction
Wide resection of ESTS in the proximal or mid-thigh results in defects that can frequently be reconstructed with locoregional flaps. Local fasciocutaneous flaps and pedicled muscle or myocutaneous flaps are both reasonable options. The pedicled rectus abdominis flap with a vertically (vertical rectus abdominis musculocutaneous), obliquely, or transversely (TRAM) oriented skin paddle can reconstruct a variety of defects in the anterior, medial, or lateral proximal thigh. Additional muscle flaps commonly used in this region are the gracilis, rectus femoris, sartorius, and vastus lateralis. The anterolateral thigh (ALT) flap is our preferred fasciocutaneous option for coverage of defects in the anterior or medial proximal thigh. In the posterior proximal thigh, soft tissue reconstruction with gluteus muscle or biceps femoris muscle flaps are frequently used.
In the mid-thigh, muscle flap options for anterior, medial, and lateral defects still include the rectus femoris, vastus lateralis, sartorius, and gracilis, with the addition of the vastus medialis and adductor longus muscles. The ALT flap is the primary fasciocutaneous option for the mid-thigh; keystone flaps and free-style propeller flaps can also be designed to reconstruct a variety of mid-thigh defects. Posteriorly, the biceps femoris and semimembranosus are the best local options for reconstruction.
Free flap soft-tissue reconstruction
Recurrent tumors, large tumors, and radiation often result in defects requiring free tissue transfer for reconstruction after resection. In a prior series of ESTS cases over 20 years published by the senior author, free-flap reconstruction was necessary in ∼ 30% of proximal and mid-thigh wounds. A variety of options exist. Most studies have not demonstrated significant differences in outcomes based on free flap choice. , , Donor- and recipient-site considerations should guide flap selection. These include the required pedicle length for anastomoses, donor morbidity, and the defect depth/size.
For large defects, the lastissimus dorsi (LD) and rectus abdominis are the commonly used free muscle flaps. Both can be harvested with a skin paddle. The contralateral ALT and parascapular flap are reliable free fasciocutaneous flaps. Both can be harvested to include muscle if dead-space obliteration is required. In addition, the subscapular and lateral femoral circumflex arterial systems (LFCA) enable harvesting of large chimeric flaps for composite tissue replacement, when indicated. Whenever possible, our preference is to avoid flaps from the contralateral lower extremity that have any functional morbidity to avoid downgrading the healthy limb.
Distal thigh, knee, and popliteal regions
Locoregional soft-tissue reconstruction
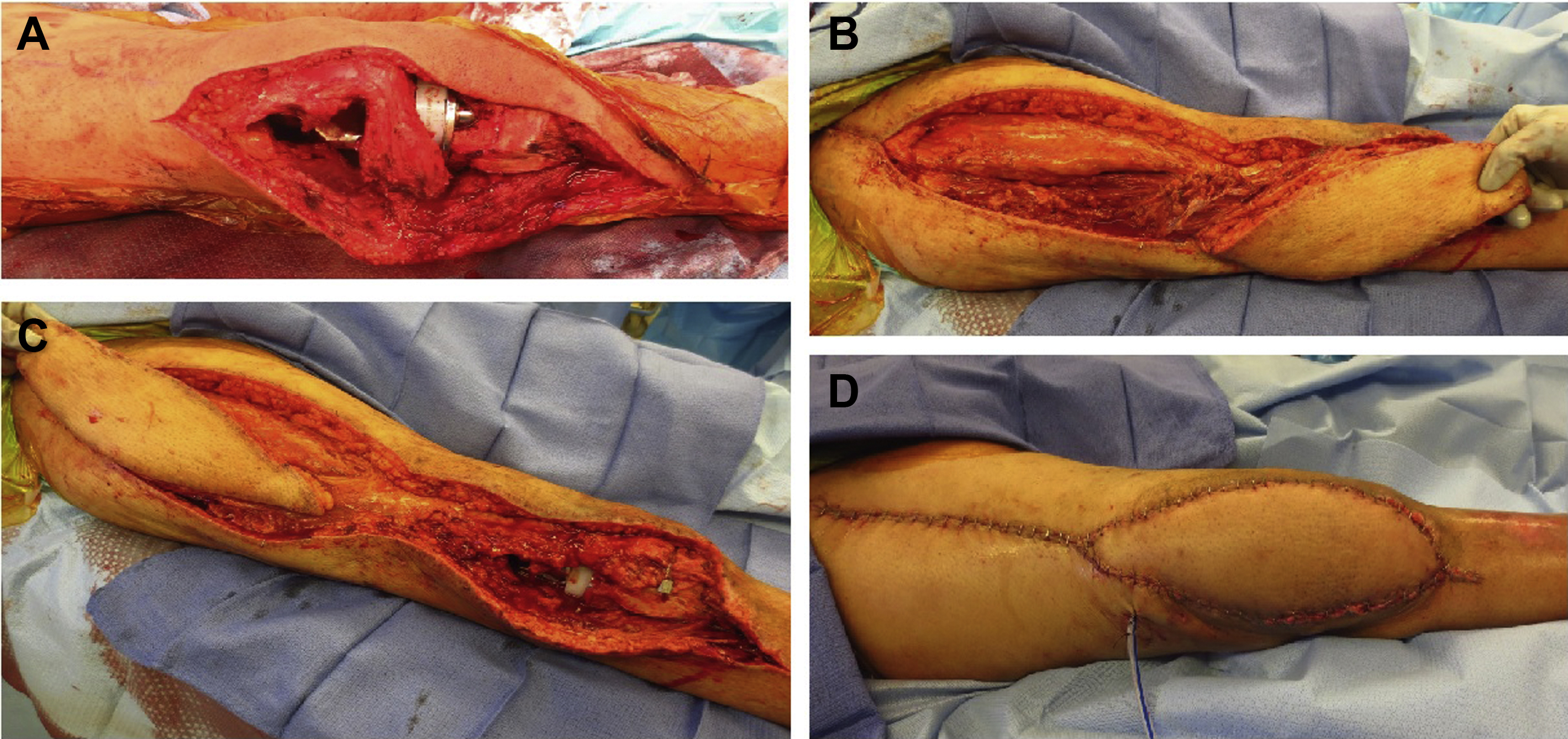
In the distal thigh, locoregional flap choices are limited. The workhorse local flaps are the reverse ALT and gastrocnemius muscle flap. The reverse ALT flap can cover a variety of defects in the distal thigh and peripatellar region ( Fig. 4 ). During flap harvest, it is important to confirm retrograde flow through the communicating branches of the distal descending LFCA and the lateral superior genicular artery. If inadequate, the flap can be converted to a standard free ALT; if venous congestion occurs, the flap can be reinset and delayed. Inclusion of tensor fascia lata can provide vascularized tissue for patellar tendon reconstruction, when indicated. The lateral or medial gastrocnemius can be used; in general, the medial gastrocnemius provides better coverage of larger and/or more proximal defects. The arc of rotation and proximal reach of the gastrocnemius flap can be improved by using a posterior midline approach and dissecting off the pes anserinus and/or medial condyle.
Free flap soft-tissue reconstruction
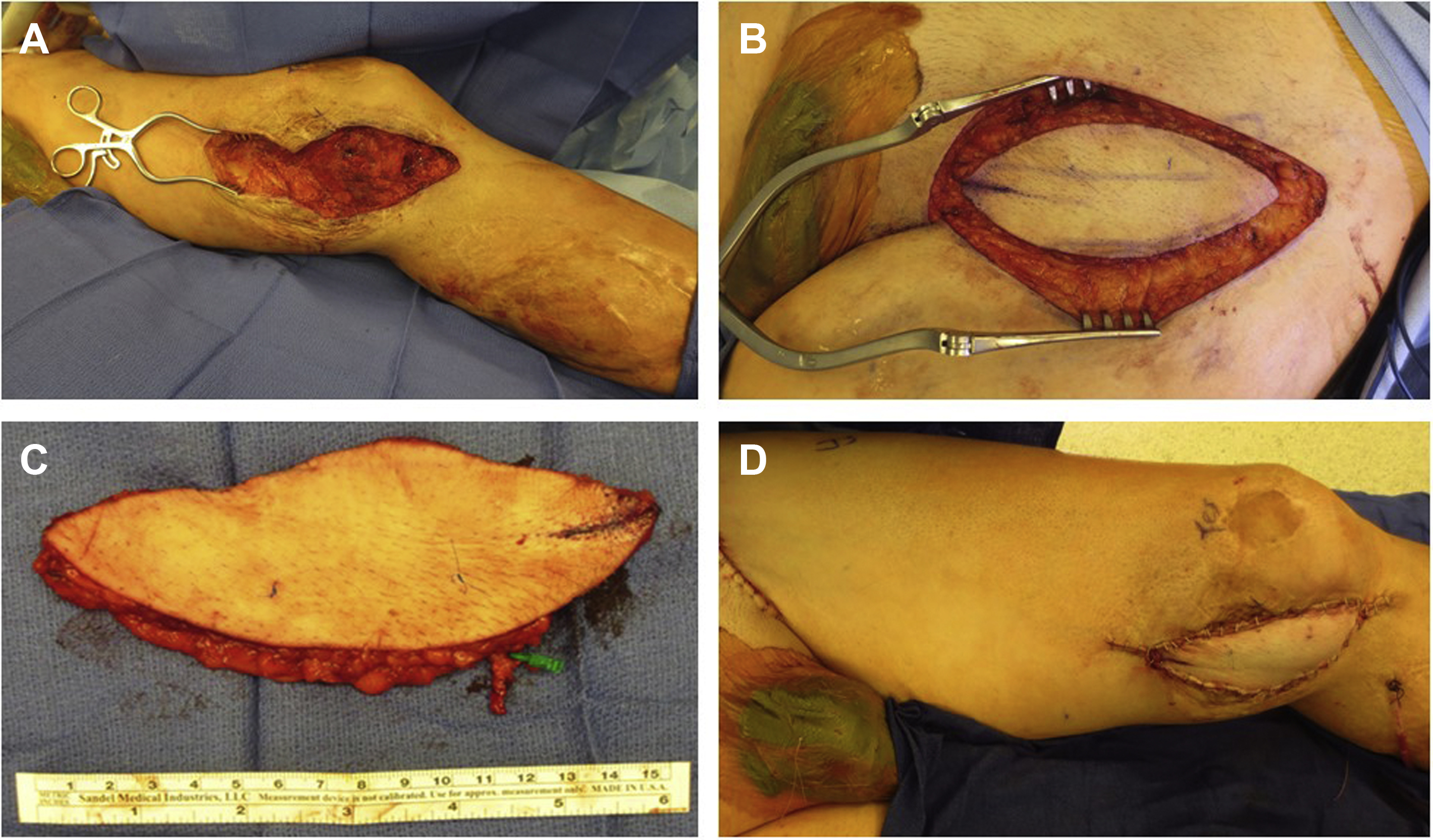
In distal thigh defects, the ALT, TRAM, and latissimus dorsi free flaps are good options for large defects. For smaller defects, options include the free gracilis, radial forearm, parascapular, lateral arm, and superficial circumflex iliac artery perforator (SCIP) flaps ( Fig. 5 ). One of the challenges to reconstruction in the distal thigh/knee is the potential lack of adequate recipient vessels for microvascular anastomosis near the zone of reconstruction. In these situations, an arteriovenous (AV) loop can be created proximally in the thigh using the femoral system, and flap vessels can be anastomosed safely to the AV loop ( Fig. 6 ).
Related posts:
 Propeller Flaps in Lower Extremity Reconstruction
Propeller Flaps in Lower Extremity Reconstruction
 The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
 Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
 Microsurgical Reconstruction of the Lower Extremity in the Elderly
Microsurgical Reconstruction of the Lower Extremity in the Elderly
 Orthoplastic Approach to Lower Extremity Reconstruction
Orthoplastic Approach to Lower Extremity Reconstruction
 Lower Extremity Reconstruction in the Pediatric Population
Lower Extremity Reconstruction in the Pediatric Population
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


