Laser (or light) hair removal, also referred to as photoepilation , is the most commonly used laser or light-based cosmetic medical procedure. The extended theory of selective photothermolysis is the basic principle for destruction of hair follicles using light. In this type of laser application the chromophore is follicular melanin. Several types of lasers and light sources have been effective for hair reduction, including the ruby, alexandrite, diode, and neodymium:yttrium-aluminum-garnet lasers and broadband, intense pulsed light sources. This article provides a broad overview of how hair can be removed using light, with an emphasis on practical considerations.
Key Points
- •
Photoepilation is based on the extended theory of selective photothermolysis, which aims to destroy follicular cells via heat. Follicular melanin is the target chromophore that locally converts the treatment light into heat.
- •
Different types of laser or light systems are available for photoepilation. Commonly used options include the alexandrite, diode, or long-pulsed Nd:YAG lasers and intense pulsed light (IPL) devices.
- •
For best results and least side effects, appropriate selection of parameters and patients is essential. The four most important treatment parameters to consider are fluence, pulse duration, wavelength, and spot size.
Introduction
Cultural and sociologic norms dictate that hair growth not only should be luxuriant and healthy but also must appear only in certain specific body sites according to gender roles. Removal of hair that is not supposed to be visible at certain sites has been performed by peoples of different cultural backgrounds all over the world for centuries. Like clothing fashions, preferences for displaying or removing hair can change dramatically over time. With occasional exceptions, such as pseudofolliculitis barbae, acne keloidalis, pilonidal sinus, trichiasis, and hidradenitis suppurative, hair removal is driven almost exclusively by personal preferences and societal pressures rather than being medically necessary. Social customs also influence whether a given hair removal process should preferably be long-term (ie, permanent) as opposed to temporary. For example, the daily ritual of removing facial hair temporarily becomes a rite of passage among maturing adolescent men, and for the rest of their lives men are more or less conditioned to dutifully attend to this practice to varying degrees without ever wishing that their facial hair be permanently gone. In contrast, body hair among men is no longer the preferred esthete, with a corresponding demand by both sexes for smooth bodies. A range of physical, chemical, and pharmacologic approaches exist for dealing with unwanted hair, and most deliver excellent short-term results. The development of lasers and other high-intensity light sources for removing hair, also known as photoepilation , has raised the realistic specter of effective and efficient long-term hair removal and is the focus of this review. The extent to which light-based hair removal remains a medical procedure will depend largely on the development of devices that can be used safely by consumers without the need for physician supervision. In this article, unless otherwise specified, the term light when used alone without qualification refers collectively to lasers and other (ie, nonlaser) high-intensity sources.
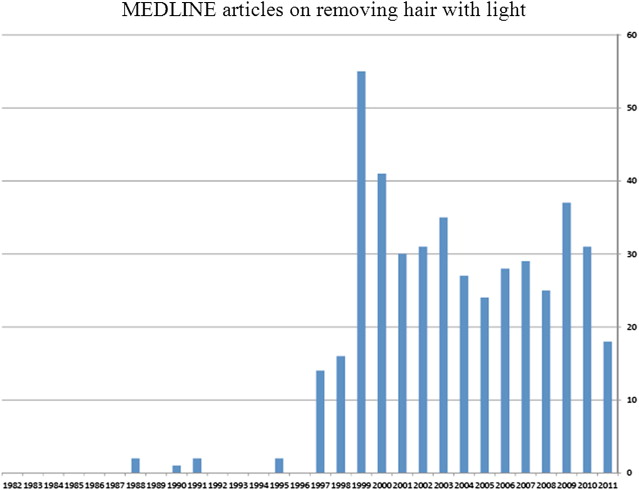
Once the principle of selective photothermolysis for highly targeted therapy was proven via the effective destruction of port wine stain blood vessels using pulsed lasers, it was only a matter of time until the hair follicle could be similarly targeted. The initial systematic approach to laser hair removal used millisecond ruby laser pulses with the goal of achieving permanent effects. Prior studies on laser hair removal had focused on medically abnormal hair growth, such as pilonidal sinuses. In 1996, the U.S. Food and Drug Administration (FDA) approved the use of lasers for removing hair, and since then hair removal has grown to become the most common medical application of high-intensity photonic devices. The transformation of the hair removal industry since the mid-1990s is paralleled by an extensive literature documenting the exploration of dosimetry, novel devices, and clinical methods for using this technology ( Fig. 1 ).
The FDA permits device companies to claim permanent reduction , but not permanent removal of hair for their lasers or intense light sources. Permanent hair reduction is defined as the long-term, stable reduction in the number of hairs regrowing after a treatment regime, which may include several sessions, but does not necessarily imply that all hairs within the treatment area are eliminated.
More specifically, the number of regrowing hairs must be stable over a period greater than the duration of the complete growth cycle of hair follicles, which varies from 4 to 12 months according to body location. Mechanistically, the energy required to induce thermal follicular destruction is mediated through the photobiologic targeting of melanin within the hair follicle complex.
Introduction
Cultural and sociologic norms dictate that hair growth not only should be luxuriant and healthy but also must appear only in certain specific body sites according to gender roles. Removal of hair that is not supposed to be visible at certain sites has been performed by peoples of different cultural backgrounds all over the world for centuries. Like clothing fashions, preferences for displaying or removing hair can change dramatically over time. With occasional exceptions, such as pseudofolliculitis barbae, acne keloidalis, pilonidal sinus, trichiasis, and hidradenitis suppurative, hair removal is driven almost exclusively by personal preferences and societal pressures rather than being medically necessary. Social customs also influence whether a given hair removal process should preferably be long-term (ie, permanent) as opposed to temporary. For example, the daily ritual of removing facial hair temporarily becomes a rite of passage among maturing adolescent men, and for the rest of their lives men are more or less conditioned to dutifully attend to this practice to varying degrees without ever wishing that their facial hair be permanently gone. In contrast, body hair among men is no longer the preferred esthete, with a corresponding demand by both sexes for smooth bodies. A range of physical, chemical, and pharmacologic approaches exist for dealing with unwanted hair, and most deliver excellent short-term results. The development of lasers and other high-intensity light sources for removing hair, also known as photoepilation , has raised the realistic specter of effective and efficient long-term hair removal and is the focus of this review. The extent to which light-based hair removal remains a medical procedure will depend largely on the development of devices that can be used safely by consumers without the need for physician supervision. In this article, unless otherwise specified, the term light when used alone without qualification refers collectively to lasers and other (ie, nonlaser) high-intensity sources.
Once the principle of selective photothermolysis for highly targeted therapy was proven via the effective destruction of port wine stain blood vessels using pulsed lasers, it was only a matter of time until the hair follicle could be similarly targeted. The initial systematic approach to laser hair removal used millisecond ruby laser pulses with the goal of achieving permanent effects. Prior studies on laser hair removal had focused on medically abnormal hair growth, such as pilonidal sinuses. In 1996, the U.S. Food and Drug Administration (FDA) approved the use of lasers for removing hair, and since then hair removal has grown to become the most common medical application of high-intensity photonic devices. The transformation of the hair removal industry since the mid-1990s is paralleled by an extensive literature documenting the exploration of dosimetry, novel devices, and clinical methods for using this technology ( Fig. 1 ).
The FDA permits device companies to claim permanent reduction , but not permanent removal of hair for their lasers or intense light sources. Permanent hair reduction is defined as the long-term, stable reduction in the number of hairs regrowing after a treatment regime, which may include several sessions, but does not necessarily imply that all hairs within the treatment area are eliminated.
More specifically, the number of regrowing hairs must be stable over a period greater than the duration of the complete growth cycle of hair follicles, which varies from 4 to 12 months according to body location. Mechanistically, the energy required to induce thermal follicular destruction is mediated through the photobiologic targeting of melanin within the hair follicle complex.
Excessive or unwanted hair growth
Excessive hair growth can perhaps be distinguished from unwanted hair largely by the notion that “unwanted hair” refers specifically to a subjective patient expectation, whereas “excessive hair” growth implies either a significant deviation from normal physiology or a pathologic process. Excessive hair growth is usually also unwanted by patients, but no question exists that a large proportion of patients who have unwanted hair have absolutely no physiologic or pathologic hair excess. In these cases, the unwanted hair is fundamentally a cosmetic concern. Racial variations in normal hair pigmentation and growth can be the source of unwanted hair, particularly for women.
Pathologically excessive hair growth can be classified to 2 groups: hypertrichosis and hirsutism.
Hypertrichosis
Hypertrichosis generally refers to diffuse or localized hair growth in androgen-independent areas of the body. Hypertrichosis develops when vellus hairs convert to terminal hairs. Diffuse hypertrichosis may be caused by medications, anorexia nervosa, or genetic, developmental, and metabolic disorders.
Hirsutism
Hirsutism is defined as excessive terminal hair growth in androgen-dependent areas of face or body of women, including the lip, sideburn area, chin, and chest. Hirsutism affects 5% to 15% of women, and is usually related to qualitative changes in hair fiber, such as diameter, pigmentation, and length, rather than the number of hair follicles. The hair count is genetically determined and the number of hair follicles depends on factors such as race and ethnicity. Hirsutism affects quality of life and can induce anxiety, depression, embarrassment, low self-confidence, and body dissatisfaction. In hirsutism treatment, the goals are destruction of the hair follicle and/or reduction in the hair shaft caliber.
Polycystic ovary syndrome is the most common cause of androgen overproduction. Adrenal hyperplasia, hyperandrogenic insulin-resistant acanthosis nigricans syndrome, androgen-secreting tumors and androgenic drug intake are less frequent causes. Idiopathic hirsutism is caused by increased sensitivity of hair follicles to normal levels of circulating androgen and/or increased peripheral conversion of testosterone to dihydrotestosterone by 5α-reductase.
Laser and light biophysics and hair removal
The extended theory of selective photothermolysis is the principal mechanism of laser hair removal. Melanin in the hair shaft, outer root sheath of infundibulum, and matrix is the main chromophore for laser hair removal. Melanin as a chromophore absorbs certain wavelengths in the red and infrared parts of the electromagnetic spectrum. After laser beam energy is absorbed, it transforms to heat in the tissue and causes damage to the hair follicle. For permanent hair removal, follicular stem cells in the bulge region and/or dermal papilla should be destroyed by heat diffusion from the melanin to the stem cells. Because the actual chromophore and target are not identical, the pulse duration should be longer than the chromophore thermal relaxation time to conduct heat diffusion to hair follicle stem cells. Because of the relative or absolute absence of melanin within light-colored, red, gray, white, or vellus hair, photon absorption is insufficient to cause photothermal follicular alteration. Dark hair on a background of light skin represents the best target for treatment.
Optimizing Hair Removal Via Skin Cooling
To remove unwanted hairs from any given area, light must pass through the epidermis and then be absorbed by target hair follicles in the dermis. During laser hair removal, the delivered fluence at the skin surface must be high enough so that sufficient photons are delivered to and absorbed at the depth of the follicle to cause irreversible damage to the hair-producing apparatus. Melanin within the interfollicular epidermis competes with hair follicle melanin for laser energy absorption. When the epidermal temperature is 45°C or greater, epidermal thermal damage can occur. If the heat produced within the epidermis can be dissipated or prevented from exceeding the 45°C threshold, the risk of damage will be decreased. Therefore, cooling the skin surface, especially in darker skin types, can decrease epidermal thermal damage and minimize laser-induced side effects. Cooling also permits treatment with higher fluences, thereby increasing the overall effectiveness of laser hair removal.
Photoepilation devices for hair removal ( Table 1 )
Ruby
Long-pulsed ruby lasers were the first laser used for hair removal. A xenon flash lamp excites a ruby crystal that emits a laser beam of 694 nm. Ruby lasers are indicated in Fitzpatrick skin types I through III with dark hair. Primarily because of their relative inefficiency and high cost, ruby lasers are no longer commercially available in North America.
| Wavelength | Pulse Duration (ms) | Fluence (J/cm 2 ) | Spot Size (mm) | |
|---|---|---|---|---|
| Ruby | 694 | No longer commercially available in North America | ||
| Nd:YAG | 1064 | 0.1–10000 | Up to 900 | 1.5–30 x 30 |
| Diode | 800–810 | 5–500 | Up to 100 | 5–22 x 35 |
| Alexandrite | 755 | 0.1–300 | Up to 600 | 1.5–18 |
| IPL | 400–1400 | 0.3–500 | Up to 500 | Up to 50 x 25 |
Neodymium:Yttrium-Aluminum-Garnet
Initially, the Q-switched neodymium:yttrium-aluminum-garnet (Nd:YAG) laser was used in combination with a carbon particle suspension that was applied topically to the skin before laser treatment. Subsequently, the carbon suspension was shown to be not necessary and that long-pulsed rather than ultrashort Q-switched pulsed lasers were more effective for hair removal. The long-pulsed Nd:YAG laser is best indicated for patients with Fitzpatrick skin phototype VI. The Nd:YAG laser system operates at a longer wavelength (1064 nm) than the alexandrite laser, allowing deeper penetration into the dermis. The Nd:YAG laser is less absorbed by epidermal melanin, and therefore is possibly more suitable for darker skin types because of lesser side effects in these patients. Clinical studies have shown less hair removal with the Nd:YAG laser than with the ruby or alexandrite lasers.
Alexandrite
The long-pulsed alexandrite (755 nm) laser has been shown to be effective for hair removal. Patients with Fitzpatrick skin phototypes I through IV can be treated with long-pulse alexandrite lasers.
Diode
The long-pulsed diode laser has been used for laser hair removal, and is recommended for patients with Fitzpatrick skin phototypes I through V. Multiple arrays of semiconductor diodes provide a laser light of 800 to 810 nm. Diode lasers are generally considered reliable devices.
Nonlaser Devices
Intense pulsed light (IPL) devices emit polychromatic noncoherent light with wavelengths ranging from 400 to 1400 nm. With these light sources, different filters are used to target different chromophores. The light delivery systems for IPLs consist of broad rectangular crystal probes that are held in contact with the skin. Good alignment of each adjacent rectangular exposure pulse and maintenance of skin contact over the entire crystal surface are important for uniform treatment.
Radiofrequency Combined with IPL
Dual-energy technology is based on the delivery of synchronous pulses of bipolar radiofrequency current and pulsed visible light within the same pulse to reduce the light intensity and side effects.
Photoepilation techniques
Patient Preparation and Selection
Before treatment, patient evaluation should focus on identifying treatable causes of hirsutism or hypertrichosis, reviewing previously used methods for hair removal and checking for a history of herpes labialis or genitalis if perioral or pubic areas are to be treated. The informed consent process should include a review of potential complications, such as blistering and crusting, and side effects such as hypopigmentation, hyperpigmentation, scarring, keloid formation, paradoxical hypertrichosis, and infection. In addition, patients must have realistic expectations of what is possible with light-based hair removal, particularly the fact that these procedures lead to long-term reduction of hair but not necessarily complete and permanent removal. Patients should be informed that lasers are less effective for treating vellus hair or hair that is light-colored, red, gray, or white.
For up to 6 weeks before and after treatment, patients should use a broad-spectrum sunscreen and avoid tanning or applying sunless tanners. They should also avoid plucking, waxing, or electrolysis 2 weeks before treatment, because this can make it difficult to visualize and delineate the target sites during treatment. Relative contraindications to using light to remove hair include gold therapy, isotretinoin therapy in the previous 6 months, photosensitizing drugs, pregnancy, and photosensitive disorders. In darker skin patients, test spot treatments are often appropriate for determining the appropriate laser parameters and also predicting the degree to which postinflammatory dyspigmentation may occur. Other situations that warrant caution include patients who have disorders that may koebnerize (eg, vitiligo, psoriasis) or who have a tendency to form keloids.
Anesthesia and Pain Control
Topical anesthetics reduce pain for laser hair removal. There is no difference between lidocaine and EMLA cream for pain control in laser hair removal. Therefore, cost and potential side effects are important factors in selecting the appropriate anesthetic. One to 2 hours before the laser treatment, a topical anesthetic cream may be applied and covered to reduce pain. Moistened gauze can be used to cover the skin after applying topical anesthetic to maximize its effects and ensure its adherence to the target sites. Topical piroxicam and EMLA provided similar pain relief in female patients after 1064-nm Nd:YAG laser-assisted hair removal. Topical piroxicam has fewer inflammatory side effects. Various skin-cooling systems also reduce pain and discomfort. Pneumatic skin flattening (PSF) technology is believed to reduce pain by invoking the “gate theory” of pain transmission (see later section on “vacuum-assisted treatment”).
Primary Laser and Light Treatment Parameters
There are 4 main parameters to consider when using lasers and light: wavelength, fluence, spot size, and pulse duration. The wavelength is usually fixed according to the specific device type, whereas the operator selects the fluence, spot size, and pulse duration.
Wavelength
Melanin within the hair shaft is the chromophore for laser hair removal. Although melanin is absorbed by all wavelengths throughout the ultraviolet, visible, and near-infrared (NIR) regions, only the longer-wavelength photons (ie, red to NIR) are capable of penetrating the skin to the level of the growing hair follicle. NIR lasers may be associated with a lower risk of skin dyspigmentation after treatment because of their lower absorption by epidermal melanin compared with red photons.
Spot size
The spot size is the diameter of the laser beam or the overall linear dimensions of the IPL skin contact probe. Because of the phenomenon of lateral scattering of light once it penetrates the skin, the spot size has an effect on the effective depth of light penetration. If all other parameters are held constant, a larger spot size will result in an overall greater depth of effect, which is desirable for targeting hair follicles.
Pulse duration
Pulse duration refers to the subsecond duration of each light exposure, and is inversely proportional to the peak power density of the laser or light pulses. According to the theory of selective photothermolysis, thermal effects within tissue can be confined to a specific structure through heating that structure faster than it cools. The rate at which any tissue component cools is largely dependent on the square of its physical diameter and is usually specified by its thermal relaxation time, which in turn is the time it takes for the target to dissipate half of its heat to the surrounding tissue. To achieve selective photothermolysis, the optimal pulse duration is roughly equal to or shorter than the thermal relaxation time.
Hair-bearing skin contains melanin as a chromophore both within the hair shaft and the interfollicular surface epidermis. During laser hair removal, epidermal melanin represents an unintended bystander target. Clinical effects on the epidermis can be minimized through selecting pulse durations that are longer but do not exceed the follicular thermal relaxation time. Longer pulse durations allow for more gentle heating of the epidermis by slowing the deposition of the light energy into the skin; the more gradually the pigmented epidermis absorbs light, the slower its conversion to heat, making cooling more efficient and limiting any deleterious thermal effects on the interfollicular epidermis. This mechanism is essentially an extension of the concept of selective photothermolysis, and has been referred to as thermokinetic selectivity , which states that smaller structures (eg, epidermal melanin) will lose heat more quickly than larger structures (eg, dermal hair follicles). The pulse durations in laser and light devices have a range from 1 to 600 ms; usually pulse durations longer than 100 ms are preferred in darker skin types.
Fluence
The amount of energy delivered to a unit area in a single pulse is defined as fluence. Higher fluences deliver more photons to the hair follicle, and therefore higher energy results in more hair reduction. However, the risk of inducing side effects will be increased with higher fluences. Some authors recommend test treatment spots to determine suitable energy and pulse duration settings, particularly in dark-skinned patients. The test spot should be selected to match with the treatment area in terms of skin color and hair density. From a practical point of view, the fluence should be gradually titrated upward until the clinical threshold of immediate perifollicular erythema and edema is reached; this determines the appropriate optimal fluence setting. Another useful immediate treatment end point is whether hairs within the treatment site can be easily pulled and released from the skin using epilating forceps. The fluence should be gradually increased until this is observed.
Secondary Parameters and Techniques for Photoepilation
Skin cooling
A variety of techniques for skin cooling have been devised to lower the epidermal temperature through direct contact (ie, aqueous gel or chilled transparent optical handpiece tips) or the delivery of cold air or cryogen sprays to the skin surface. Aggressive cooling with cryogen spray and cold air has been associated with blistering and discoloration of the skin.
Scanners
Many laser hair removal systems are equipped with automated scanners that will direct a series of laser pulses uniformly over defined treatment areas. This feature is important for increasing treatment efficiency, especially when treating broader areas such as the back, chest, or extremities.
Vacuum-assisted treatment
Vacuum-assisted hand pieces are currently featured in diode lasers and work by stretching the skin through suction, which essentially positions the hair follicle closer to the skin surface. The stretched epidermis also means that the laser energy is distributed over a larger area, such that the density of epidermal melanin and heating within that layer are reduced. This handpiece design is promoted as being capable of removing hair at lower fluences and greater coverage rates.
PSF technology decreases pain based on Melzack and Wall’s “gate theory” of pain transmission, in which activation of nerves that do not transmit pain signals interferes with signal transmission from pain fibers. The PSF suction device stimulates the tactile and pressure receptors on skin before the laser pulse and blocks the transmission of pain. PSF also decreases blood flow in dermal vessels, removing a competing chromophore from the treatment area. PSF has reduced pain associated with hair removal by laser or IPL.
Frequency and Number of Treatments
Multiple laser treatments are necessary to achieve long-term reduction of hair, typically in the range of 5 to 7 sessions spaced approximately 4 to 8 weeks apart. With each session, an estimated 15% to 30% of hairs are removed. Treated hairs usually shed 2 weeks after the laser treatment. Treated sites will manifest a decrease in the total hair density with treatment and/or miniaturization of hairs.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


