Locoregional flaps play an important role in soft tissue reconstruction of the lower extremity and should be considered an effective option in soft tissue reconstruction. The medial hemisoleus muscle flap and the distally based sural artery flap can be elevated because of unique vascular anatomy and more advanced surgical techniques in flap dissection. Each flap can replace free tissue transfer as the first choice for soft tissue reconstruction of a less extensive wound in the distal third of the leg. Patient selection and detailed knowledge of the flap and its advanced technique for flap dissection are keys to success.
Key points
- •
Locoregional flaps play an important role in soft tissue reconstruction of the lower extremity.
- •
Either the medial hemisoleus muscle flap or the distally based sural artery flap can be a work horse for reconstruction of a soft tissue wound in the distal third of the leg.
- •
These flaps may be able to replace free tissue transfer as the first choice for soft tissue reconstruction of a less extensive wound in the distal third of the leg.
- •
Proper patient selection as well as a detailed knowledge of each flap anatomy and its advanced technique for flap dissection are the keys to the success.
Introduction
Locoregional flaps play an important role in the soft tissue reconstruction of the lower extremity and should also be considered as an effective and valid option in contemporary approach to lower extremity reconstruction. A study reviewed 290 lower extremity trauma patients over a 12-year period from a level 1 trauma center from a major tertiary hospital clearly showed that more local flaps and skin grafts were performed in general for soft tissue reconstruction of open tibia and fibula fracture wounds than free flaps. In addition, local flaps for soft tissue coverage of lower extremity wounds may be more cost effective than free flaps for the same soft tissue wound in selected patients.
Although free tissue transfer has become a standard choice of procedure for many soft tissue reconstructions in lower extremity reconstruction, the application of locoregional flaps for lower extremity reconstruction should be equally emphasized. Over the last 2 decades, several locoregional flaps have been refined or revisited in terms of their role in soft tissue reconstruction of the lower extremity because much more advancement in understanding of the flap anatomy and in surgical dissection of each flap has also been made. It has become clear that local or regional flaps can also safely be chosen for soft tissue coverage in the lower extremity. , This is true because of the evolution of reconstructive flap surgery, especially a wide application of several muscle flaps, fasciocutaneous flaps, or even pedicled perforator flaps. In addition, many locoregional flaps can be elevated because of their unique vascular anatomy and more advanced surgical technique in flap dissection. Several useful locoregional flaps are commonly designed in a reverse fashion and can, therefore, be used to reconstruct many complex wounds in the distal third of the leg wound as a good alternative to free tissue transfer.
When managing a complex soft tissue wound in the lower extremity, plastic surgeons can be divided into 2 general groups: microsurgeons and nonmicrosurgeons. Obviously, microsurgeons are capable of performing free tissue transfers and their preference for most lower extremity reconstructions are free flaps. In contrast, nonmicrosurgeons only can perform locoregional flaps for lower extremity reconstructions; for certain patients, they have to transfer the care to microsurgeons in the same hospital or in a different hospital because they could not perform microsurgical procedures. It is possible that proper selection of a more suitable procedure for a lower extremity reconstruction is overshadowed by a plastic surgeon’s ability and preference, but not by the actual soft tissue wound of the patient.
In this article, the author describes 2 reliable locoregional flaps, the medial hemisoleus muscle flap and the distally based sural artery fasciocutaneous flap, that have been used in his practice to manage a complex wound in the distal third of the leg. Because this author also routinely performs microvascular free tissue transfer, the selection of these 2 locoregional flaps for lower extremity reconstruction can be considered to have less bias and a free flap can be a good backup option if a locoregional flap is not successful. The indications and contraindications, preoperative evaluations, flap dissections, and management of flap-related complications are discussed as well.
Indications and contraindications
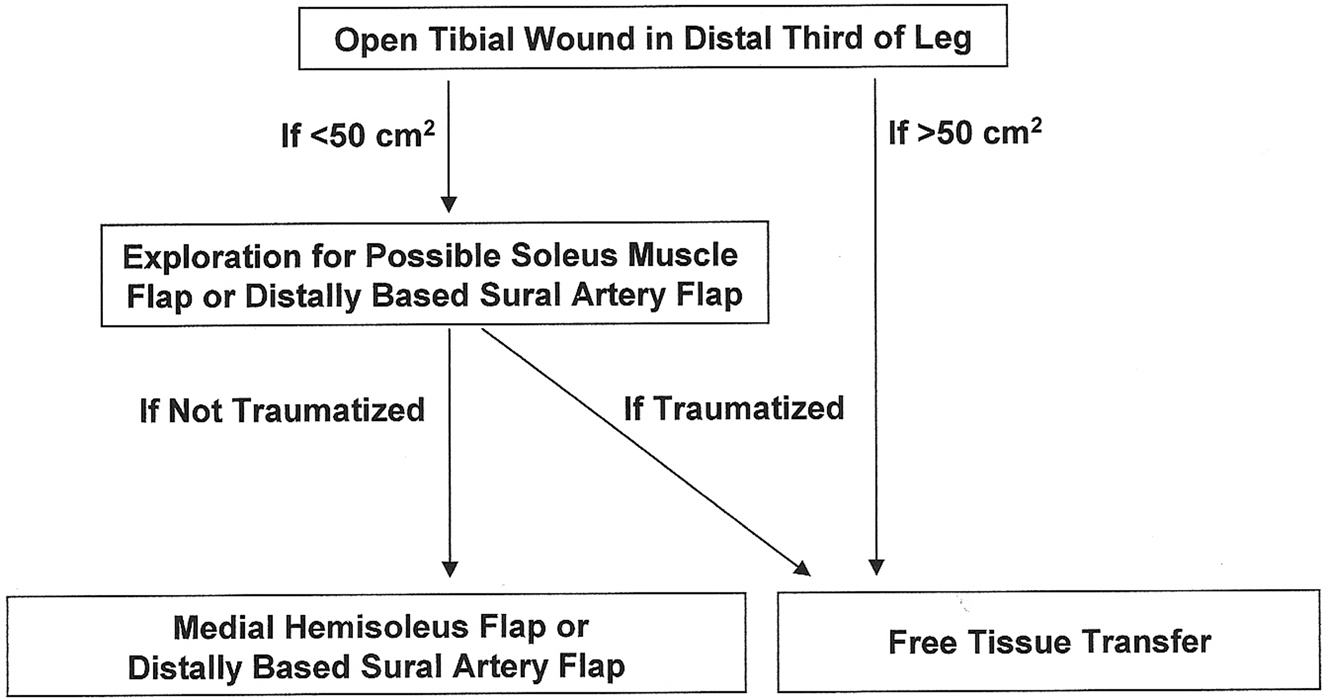
It is critical to know the indications of a locoregional flap for reconstruction of a complex wound in the lower extremity, especially in the distal third of the leg. In general, a locoregional flap can be used to cover a relatively small (<50 cm 2 ) wound in the distal third of the leg ( Fig. 1 ). Such a locoregional flap should not be within the zone of injury and should not have been traumatized from a previous injury or surgery. The surgeons should be familiar with those flaps, including advanced techniques for flap dissection. The surgeons should also feel comfortable handling complications related to locoregional flap reconstruction.
The medial hemisoleus muscle flap and the distally based sural artery flap are 2 workhorse flaps that are used by the author to reconstruct a complex wound associated with an open fracture or exposed bone in the distal third of the leg. , More recently, the concept of pedicled perforator flaps has been introduced in the literature. These axially based flaps can be elevated as a named perforator flap or even as a freestyle pedicled flap for various needs for soft tissue coverage in the lower extremity. These flaps are described separately elsewhere in this issue.
The timing for a locoregional flap lower extremity reconstruction depends on the patient’s readiness and associated medical conditions. In general, a definitive soft tissue reconstruction is commonly performed within 7 to 10 days after the initial consultation. However, because a locoregional flap is a relatively short procedure (about 2 hours) and has more straightforward postoperative care, it can be performed right after definitive bony reconstruction by orthopedic trauma service in the same operation.
Contraindications for a locoregional flap for reconstruction a complex wound in the distal third of the leg are as follows: the wound is larger (ie, >50 cm 2 ); more composite tissue involvement, the flap is within the “zone of injury,” or significant peripheral vascular disease is present. If the patient has an occluded posterior tibial artery, a medial hemisoleus muscle flap is contraindicated. If the patient has an occluded peroneal artery, a distally based sural artery flap is contraindicated. For those conditions, free tissue transfer will be a more reliable option than a locoregional flap reconstruction. If the soft tissue injury is extensive and there is a significant trauma to the area that a locoregional flap would be based on, a free flap reconstruction may provide the only option for limb salvage in these patients.
Preoperative evaluation and special considerations
A complex wound in the distal third of the leg is frequently associated with an underlying tibial fracture and successful soft tissue coverage for the open fracture site provides a critical means for primary or secondary healing of the fracture as well as for limb salvage. In general, a free tissue transfer is currently the standard procedure of choice to provide meaningful soft tissue coverage in this anatomic region of the leg because there is no good local option available for such a critical soft tissue reconstruction, at least based on the classic teaching of the past 2 decades. Controversy among plastic surgeons often remains for those complex wounds in the distal third of the leg that are relatively too small for free tissue transfer, but clearly too large for primary wound closure.
Although a free flap has been considered a standard procedure of choice for soft tissue coverage in the distal third of leg, certain patients may not be candidates for free tissue transfer because of their overall medical conditions after a multisystem trauma or they are not in compliance with proper postoperative care. It becomes clear to many plastic surgeons, including this author, that not every patient requires a free flap reconstruction as a standard procedure of choice, even for an open tibial wound in the distal third of the leg, and a few locoregional flaps may serve well for selected patients with a less extensive wound in the distal third of the leg.
With a better understanding of the flap anatomy and its blood supply, as well as refinements and innovations of the flap dissection, a few locoregional flaps can be used for the soft tissue coverage of a complex wound in the distal third of the leg. In the author’s practice, the medial hemisoleus muscle flap has been selected more than any other local muscle flaps for soft tissue coverage of a complex wound in the distal third of the leg. , , , When the size of a wound is less than 50 cm 2 , a medial hemisoleus muscle flap can be chosen primarily for soft tissue coverage if the soleus muscle is not traumatized. With the application of sound clinical judgment, the author has found that many orthopedic trauma patients who have an open tibial wound in the distal third of the leg with an open tibial fracture can be reconstructed successfully with a medial hemisoleus muscle flap based either proximally or distally for soft tissue coverage. When the selection of a medial hemisoleus muscle flap for a wound in the distal third of the leg, a proximally based flap can be chosen when a defect is relatively proximal, whereas a distally based flap can be selected when a defect is relatively distal.
The distally based sural artery flap, a distant skin island flap, , , has also been used frequently to provide soft tissue coverage for a complex wound in the distal third of the leg, if the flap donor site is available and the pedicle of the flap in the lesser saphenous vein territory is not traumatized. The flap itself provides a good skin coverage to a wound in both the medial and lateral aspects of the distal leg. However, the less optimal blood supply provided by a fasciocutaneous flap has been one of the main concerns for its routine use in soft tissue coverage of a complex wound in the distal third of the leg associated with an open tibial fracture.
Frequently, the determination of whether a locoregional flap can be selected for lower extremity wound coverage is performed in the operating room where a complex wound is more properly explored and assessed by the surgeon. Such an intraoperative assessment can provide a critical means to the surgeon to decide whether a locoregional flap can safely be selected to reconstruct a complex wound in the lower extremity. In addition, the plastic surgeon’s expertise, as well as reconstructive services provided by a hospital, can play a role in the decision-making process for the flap selection.
Surgical procedures
Medial Hemisoleus Muscle Flap
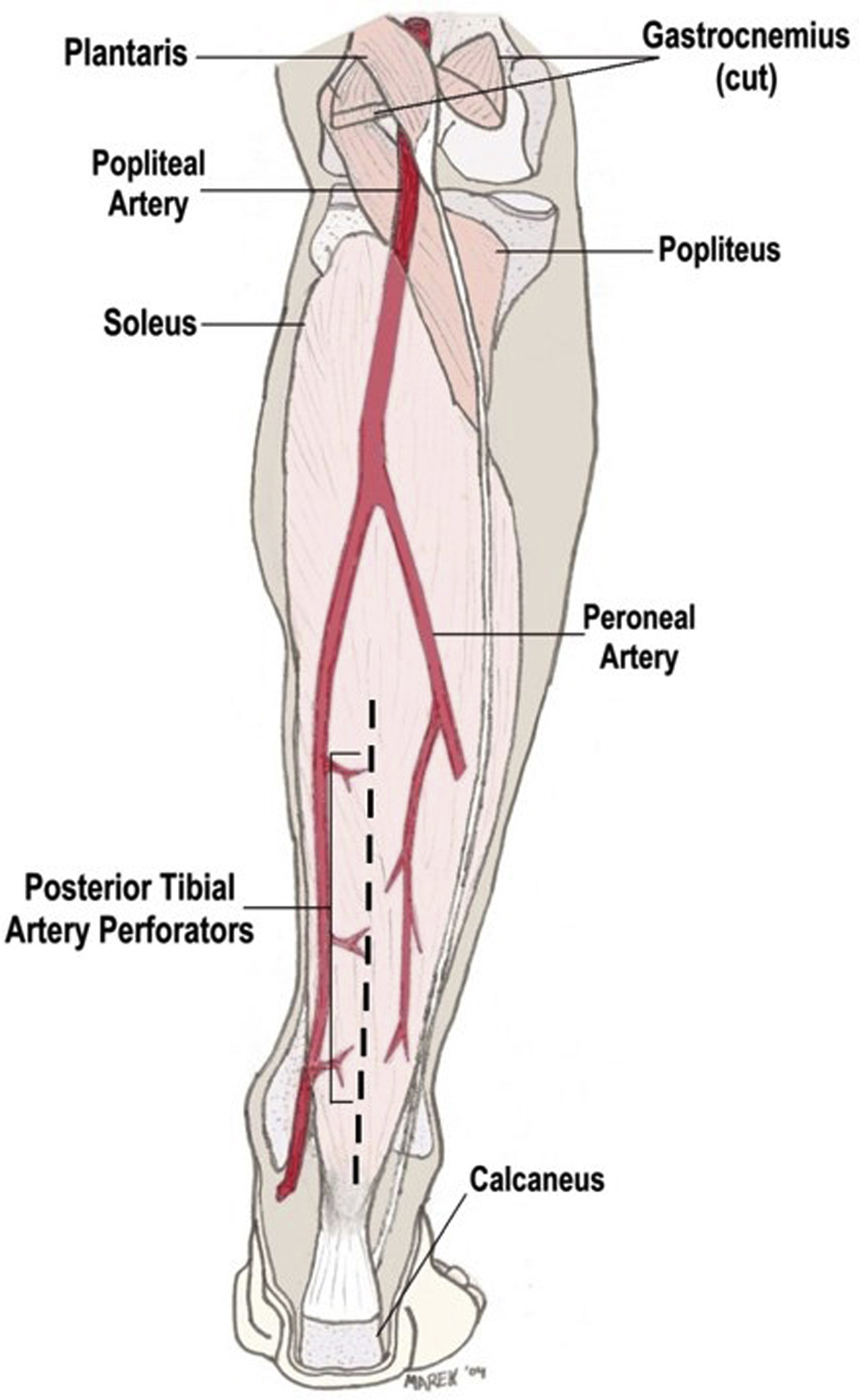
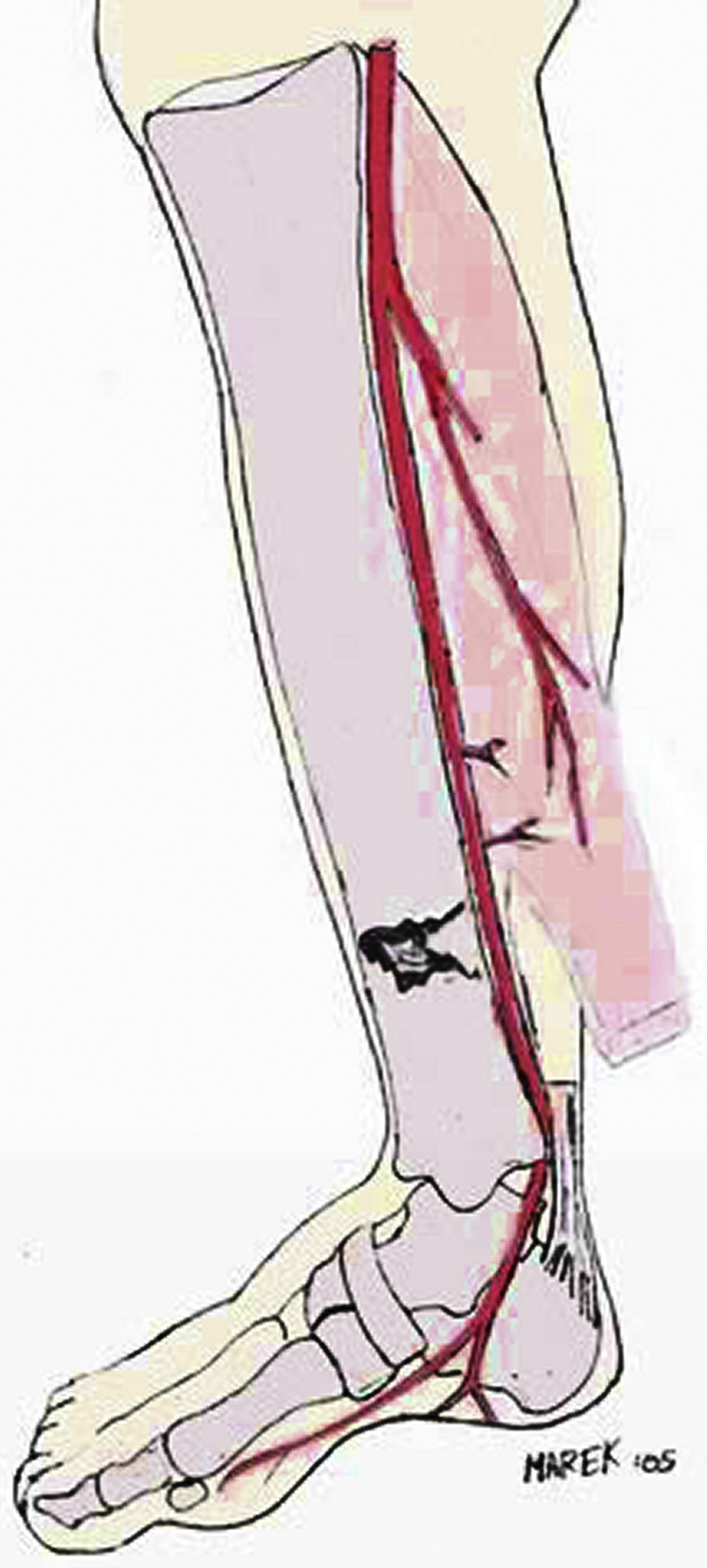
The soleus muscle is a bipenniform muscle located in the superficial posterior compartment of the leg. It originates from the fibula and medial aspect of the tibia and inserts into the calcaneus as a part of the Achilles tendon ( Fig. 2 ). The medial hemisoleus muscle flap can provide not only adequate soft tissue coverage, but can also minimize functional loss of the foot planter flexion. The bipenniform morphology of the soleus muscle and the independent neurovascular supply to either the medial or lateral belly of the muscle are important features that allow a surgeon to split the muscle longitudinally along the muscle’s midline to create a muscle flap composed of only one-half the muscle (hemisoleus). After splitting the muscle, the medial part of the muscle is supplied throughout its length by perforators arising from the posterior tibial vessels. This constant blood supply makes the medial part of the muscle (medial hemisoleus) reliable as a proximally or even distally based flap ( Fig. 3 ).

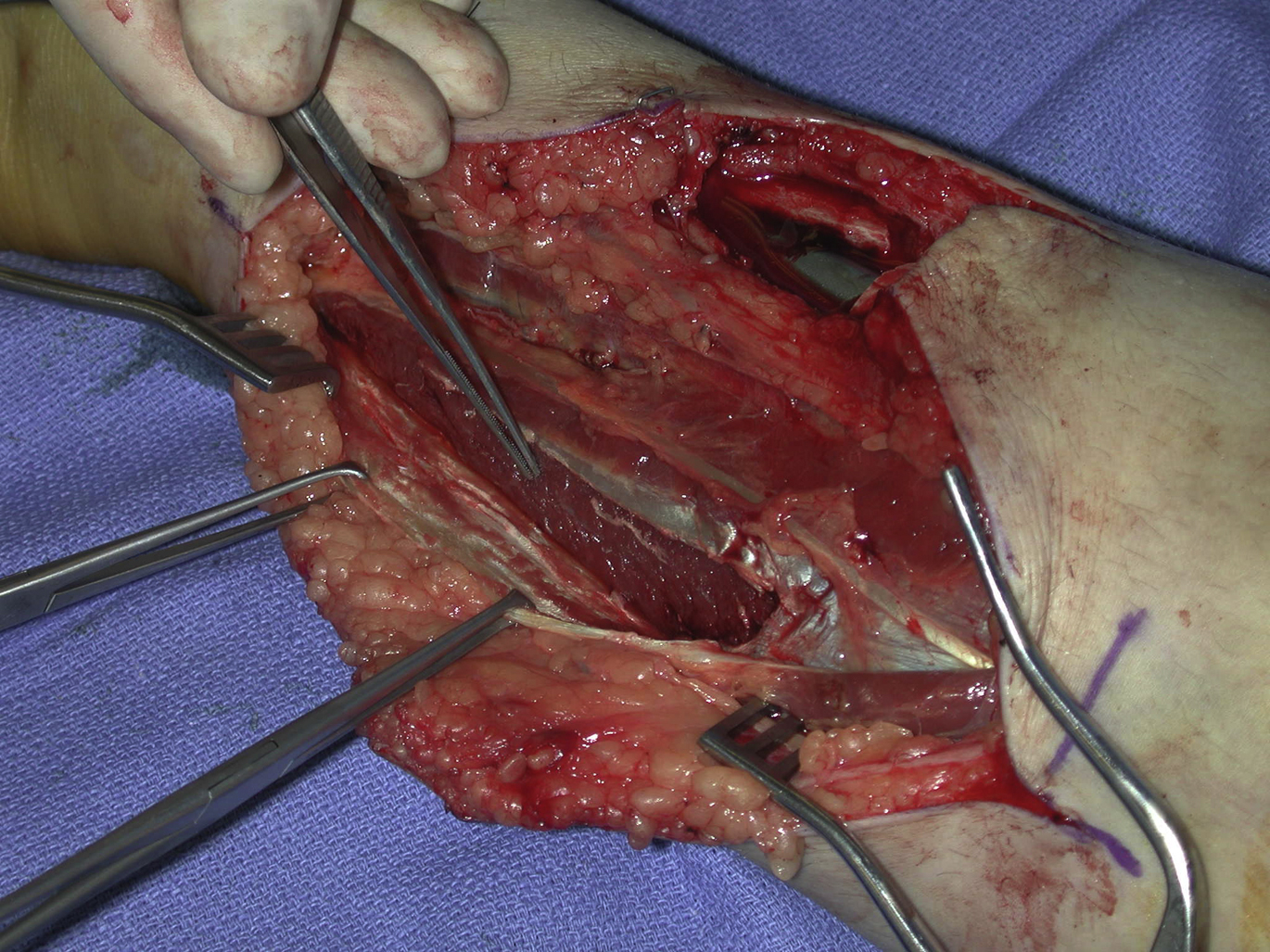
The flap dissection is done under tourniquet control. An existing wound can be extended into the incision both proximally and distally. For a proximally based medial hemisoleus muscle flap, once the medial hemisoleus muscle is identified and dissected freely from the medial gastrocnemius muscle, its insertion is divided distally at a level close to the Achilles’ tendon, depending on the length of the flap rotation required. The medial half of the muscle is split longitudinally along with a midline between the bellies of the soleus muscle. To cover a wound in the distal third of the leg ( Fig. 4 ), the proximally based medial hemisoleus muscle flap is elevated only to the level just below the junction between the middle and distal thirds of the leg with an emphasis on the preservation of as many major perforators to the flap as possible, even in the distal-third of the leg, while allowing an adequate arc of flap rotation ( Fig. 5 ). These perforators are critical sources of blood supply to the distal portion of the medial hemisoleus muscle flap and should be preserved whenever possible. During flap dissection, only the muscular portion of the soleus muscle is used as the flap; the tendinous portion of the soleus is left intact ( Fig. 6 ). The spared tendon is then approximated to the remaining lateral half of the soleus muscle with nonabsorbable sutures. This technique may minimize functional loss of the leg after the flap is harvested. With these refined techniques for the flap dissection, the flap can be suitable for a more proximal defect in the distal third of the leg.

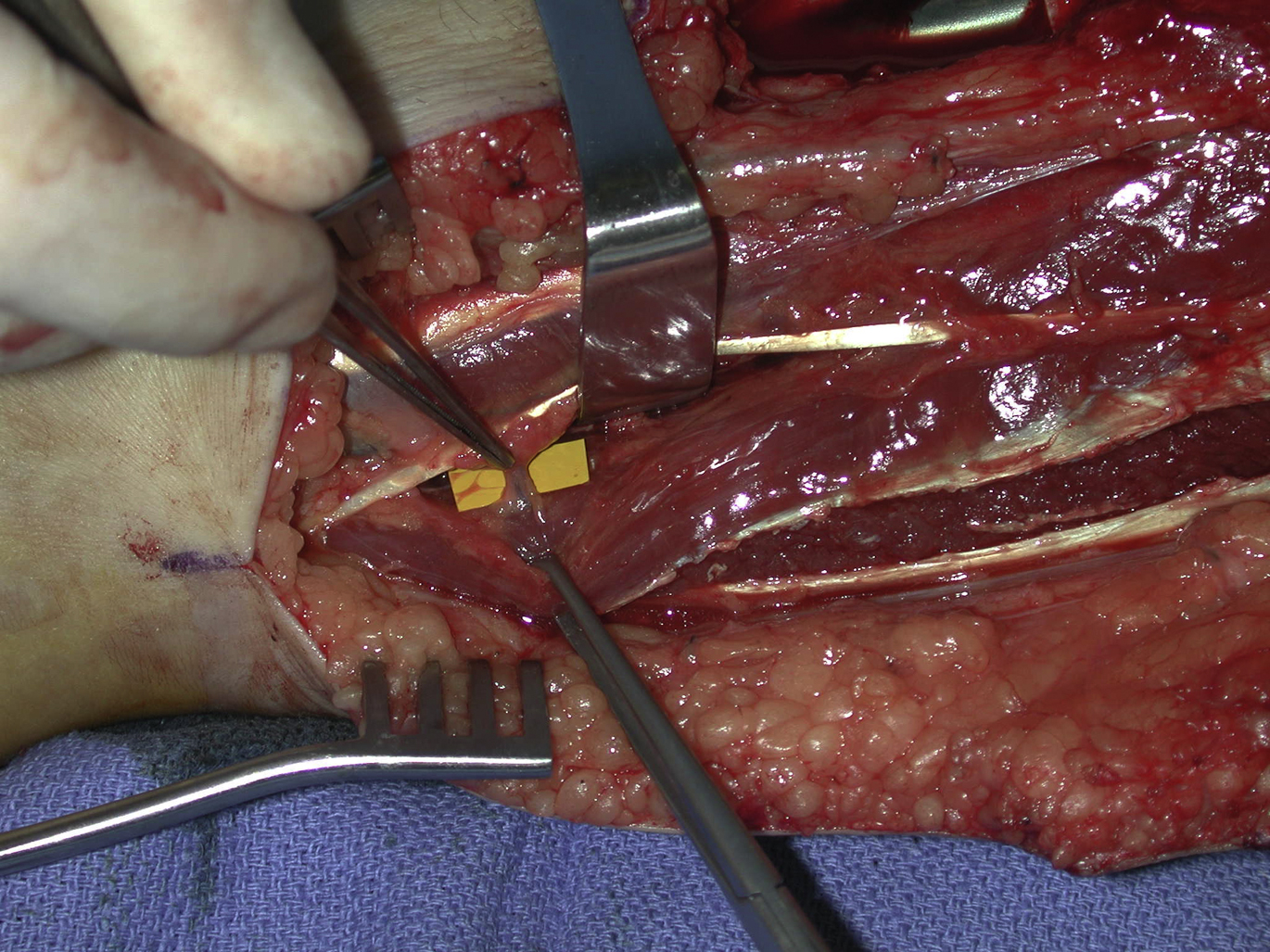
This author prefers an intraoperative dissection of the soleus muscle to confirm the level of the distal muscle insertion, although a preoperative MRI can easily identify the location of the soleus musculotendinous junction in the ankle. Once the medial hemisoleus muscle is identified and dissected freely to the level at the junction between the middle and distal thirds of the tibia, the major perforators from the posterior tibial vessels to the medial half of the soleus muscle within even distal third of the tibia should be identified ( Fig. 7 ). Next, the surgeon must be attentive in the preservation of these perforators when designing the adequate arc of flap rotation to cover the target soft tissue defect or exposed hardware ( Fig. 8 ). If needed, the medial hemisoleus muscle can be extended more laterally after longitudinally splitting, so that the flap can be made wide enough to cover a relatively large wound in the distal third of the leg. These modifications made by the author to the surgical techniques in flap dissection emphasize the preservation of an adequate blood supply to the distal portion of the medial hemisoleus muscle flap after flap elevation. These techniques maximize the reliability of the medial hemisoleus muscle flap and expand its role in reconstruction of distal third tibial wounds , , , ( Fig. 9 ).

Related posts:
 Propeller Flaps in Lower Extremity Reconstruction
Propeller Flaps in Lower Extremity Reconstruction
 Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
 Free Flaps in Lower Extremity Reconstruction
Free Flaps in Lower Extremity Reconstruction
 Orthoplastic Approach to Lower Extremity Reconstruction
Orthoplastic Approach to Lower Extremity Reconstruction
 The Anterolateral Thigh Perforator Flap
The Anterolateral Thigh Perforator Flap
 Lower Extremity Reconstruction in the Pediatric Population
Lower Extremity Reconstruction in the Pediatric Population
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


