Introduction
“It is not uncommon to find split skin grafts applied to an ulcer bed as the sole method of treatment. This can be successful, but failure is a common end result … because of a failure to treat the primary disease and an unreceptive bed of fibro-granulation tissue and/or underlying bone to support the thin split skin.” Ger first documented the usage of lower extremity muscle flaps to treat advanced stasis ulcers of the lower leg in cases where split-thickness skin graft had previously failed. He introduced vascularized muscle to prepare the wound beds for eventual skin grafting. He recognized that flexor digitorum longus, though deficient in its distal bulk, can be easily mobilized without disturbing its vascular supply to cover a variety of defects in the lower tibia.
Functional restoration of the complex and highly efficient biomechanics of the foot and ankle is a challenge for the reconstructive surgeon. Trauma, tumor ablation, neuropathy, motor dysfunction, skeletal instability, blood supply abnormalities, and immunocompromise can render the foot and ankle susceptible to breakdown. Inability to salvage the injured foot traditionally has led to major amputation, carrying with it morbid sequelae and an expensive lifetime dependence on prosthetic devices. Successful foot and ankle reconstruction demands a multidisciplinary team approach consisting ideally of a vascular surgeon skilled in endovascular and bypass techniques; a foot and ankle surgeon skilled in internal and external (Ilizarov) bone stabilization techniques; a soft tissue surgeon for soft tissue reconstructive techniques; an infectious disease specialist; and an endocrinologist. Surgical goals include ensuring a good local blood supply; debriding the wound to a clean base; correcting any biomechanical abnormality; preparing the wound for closure; closing the wound; and providing adequate off-loading to allow for healing. Reconstruction can then usually be accomplished by simple techniques 90% of the time and by complex flap reconstruction in 10% of cases. This chapter will focus on intrinsic pedicled flaps of the foot and ankle that are commonly used. Microsurgical free flaps can accomplish the same task for small defects and can fill larger defects. They do require an intact recipient vessel and a longer procedure with greater anesthetic risk. The success rates of both intrinsic muscle flaps and free flaps in the lower extremity are the same, although the complications associated with the former is twice that of the latter.
Vascular Anatomy ( Fig. 48.1 and Fig 13.7 , Fig 13.9 , Fig 13.10 , Fig 13.11 , Fig 13.15 , Fig 13.16 , Fig 13.19 )
The foot and ankle consist of six angiosomes. The following arteries feed the angiosomes of the foot and ankle: (a) the distal anterior tibial artery feeds the anterior ankle while its continuation, the dorsalis pedis artery, supplies the dorsum of the foot; (b) the calcaneal branch of the posterior tibial artery feeds the medial and plantar heel; (c) the calcaneal branch of the peroneal artery feeds the lateral and plantar heel; (d) the anterior perforating branch of the peroneal artery feeds the anterolateral ankle; (e) the medial plantar artery feeds the plantar instep; and (f) the lateral plantar artery feeds the lateral plantar midfoot and forefoot ( Fig. 48.2 ). Note that the plantar heel receives dual blood supply from the calcaneal branches of the posterior tibial and peroneal arteries. When the heel develops gangrene, this usually implies severe vascular disease involving both the peroneal and posterior tibial artery.

Because the foot is an end organ, there are many arterial–arterial anastomoses that provide a duplication of inflow. These arterial–arterial anastomoses provide a margin of safety if one of the main arteries becomes occluded. At the ankle, the anterior perforating branch of the peroneal artery is connected to the anterior tibial artery through the lateral malleolar artery. At the Lisfranc joint, the dorsalis pedis artery dives into the first interspace to connect directly with the lateral plantar artery. This vascular loop is critical in determining the direction of flow within the anterior or posterior tibial arteries, which can be antegrade or retrograde, or both. In addition, the plantar and dorsal metatarsal arteries are linked to one another at the Lisfranc joint by proximal perforators and at the web space by distal perforators. Finally, the posterior tibial artery and peroneal artery are directly connected deep to the distal Achilles tendon by 1–3 connecting arteries. Using a Doppler ultrasound probe and selective occlusion, one can determine the patency of these connections as well as the direction of flow. This is critical in designing local flaps and pedicled flap.
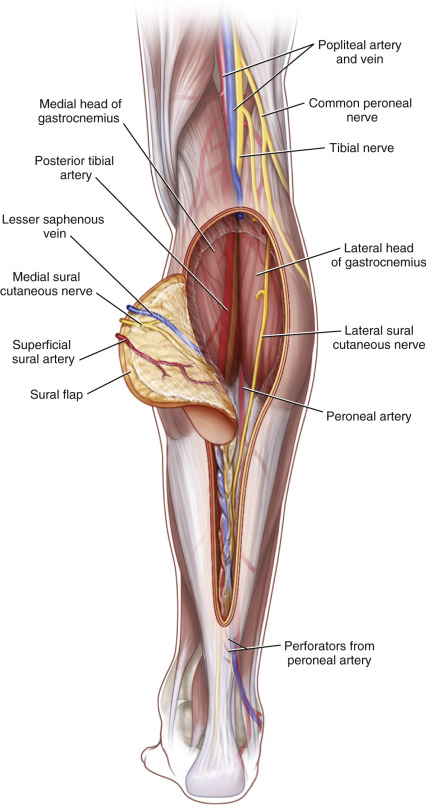
The Sural Flap
The sural flap is contained in the area of the posterior calf between the popliteal fossa and midportion of the leg. It is centered over the mid raphe between the medial and lateral heads of the gastrocnemius muscle.
Flap Anatomy ( Figs 48.1 and Fig 13.9 , Fig 13.19 )
Arterial and Venous Supply of the Flap
Dominant:
superficial sural artery
Length: 3 cm
Diameter: 1.4 mm
In a study by Leclère and colleagues, a total of 26 flaps were dissected. Of these, 50% had the takeoff of the superficial sural artery from the medial sural artery; 46% from the popliteal artery; and the remainder from the lateral sural artery. They found several perforators coming off the superficial sural artery along its course down the leg.
Minor:
perforators from the peroneal artery (retrograde flow)
Length: 1 cm
Diameter: 1 mm
Minor:
perforators from the posterior tibial artery
Length: 1 cm
Diameter: 1 mm
Minor:
neurocutaneous perforators from vasa nervorum of the sural nerve
Length: 1 cm
Diameter: 1 mm
In most cases, the arterial component is a plexus of vessels that travel along the sural nerve and receive retrograde flow from the peroneal artery perforators (3–6 perforators) 5 cm above the lateral malleolus.
Venous Drainage of the Flap ( Fig. 13.19 )
Primary:
venae comitantes of the perforating vessels named above
Length: 1 cm
Secondary:
subdermal plexus if skin is harvested
Flap Innervation ( Fig. 13.19 )
Sensory:
medial sural cutaneous nerve
Flap Components
The flap can be harvested as fasciocutaneous, fasciocutaneous with muscle, or fascia only.
Advantages
- •
A good substitute for free flap coverage of lateral, medial, and posterior ankle defects
Disadvantages
- •
Venous congestion (common)
- •
Distal necrosis of the flap
- •
Bulky (can require secondary debulking procedures)
- •
Risking a posterior myocutaneous flap for a future below knee amputation
- •
In certain patients, a delay procedure should be done prior to inset.
Preoperative Preparation
See above for general preoperative evaluation and preparation. A handheld Doppler should be used to investigate the sural artery perforators and the distal perforators from the peroneal artery in order to guide the skin paddle design.
Flap Design
Anatomic Landmarks
The skin paddle design runs from the popliteal fossa to the mid-point of the leg. Its width should be at least 3 cm but it depends on the defect.
General Thoughts About Flap Design
The most common usage for this flap is reverse sural flap to cover defects for the distal third of the leg. This distally based reverse sural artery is based on the peroneal perforators in the distal third of the flap (5–7 cm proximal to the lateral malleolus). When designing this flap, one must first determine the pivot point distally ( Fig. 48.3 ).
Special Considerations
In the current setting of perforator flaps, one can harvest and rotate the flap based on the peroneal perforator. This avoids placing a defect over the gastrocnemius muscles and risking less than an ideal donor site should the patient unfortunately go on to a below knee amputation.
Difference in Design, if Any, When Performing the Flap as Pedicled or Free
Reverse sural artery flap is used a local flap for reconstruction of distal third of the leg.
Flap Dimensions
Skin Island Dimensions
Length: average 12 cm
Width: average 6 cm
Flap Markings
The flap is outlined over the raphe between the two heads of the gastrocnemius muscle. The pedicle can be Dopplered out by tracing the lesser saphenous vein from the lateral ankle up to central raphe between the two heads of the gastrocnemius muscle ( Fig. 48.3 ).
Patient Positioning
Although the flap can be harvested in the lateral decubitus position, prone position is preferred.
Anesthetic Considerations
The harvesting of this flap should be done under general anesthesia.
Technique of Flap Harvest
The flap is outlined over the raphe between the two heads of the gastrocnemius muscle. The pedicle can be found by Dopplering the lesser saphenous vein from the lateral ankle up to central raphe between the two heads of the gastrocnemius muscle. Flap elevation begins along its proximal edge. Through this incision, the lesser saphenous vein superficial to the deep fascia and the sural nerve superficial (distal) or deep (proximal) to the fascia, is identified and ligated. The proximal sural nerve stump should be buried in the proximal gastrocnemius muscle to minimize the chances of developing a neuroma. The deep fascia, together with the above structures, is elevated with the flap. The flap pedicle edges lie 2–3 cm on either side of the lesser saphenous vein. The pedicle can be elevated with or without the overlying skin. By taking the overlying skin, one avoids placing excessive twist on the vein as it rotates 180°. The arc of rotation will provide coverage of the lateral ankle, medial ankle, and posterior heel.
Flap Modification/Flap Handling
When skin is not required, the sural flap can be harvested with fascia, only leaving the skin in place by undermining in the subcutaneous plane. If additional bulk is needed to close dead space in the defect, a part of gastrocnemius muscle can be harvested with one or two intact myocutaneous perforators that would otherwise be divided. One common complication of the reverse sural flap is venous congestion and one potential solution is to delay the flap. The flap is dissected and undermined, as described previously, but a skin bridge proximally is left intact to allow venous egress. After 7–10 days, the area of connection can be divided and the flap can be rotated into the defect.
Special Instruments
A handheld Doppler should be readily available. A thigh tourniquet can be used to achieve a bloodless field. A dermatome can be used for the harvesting of the skin graft.
Donor Site Closure and Management
A split-thickness skin graft is often used to close the donor site if skin is included in the flap. The donor site may be closed primarily if it is small or if only fascia was taken.
Technical Tips to Optimize Outcomes and Avoid Complications
- •
The venous congestion often seen with this flap can be minimized if the pedicle is harvested with 3 cm of tissue on either side of the pedicle and with the overlying skin intact.
- •
Problems with the venous drainage can be further alleviated by delaying the flap for 7–10 days after ligating the proximal lesser saphenous vein and sural artery.
- •
Supercharging of the reversal sural flap can be performed via anastomosis of the proximal end of the small saphenous vein to any vein in the receipt site.
- •
The inset of the flap is critical to avoid kinking of the pedicle. Offloading the flap and heel during the healing phase is simplified by using an Ilizarov-type frame.
Flap Usage
Pedicled
It can be rotated proximally to cover the defects of the popliteal fossa and upper third of the leg. The reverse flap reaches the ankle, heel, and foot.
Typical Indications for the Use of This Flap
- •
Ankle
- •
Posterior heel
Atypical Indications for the Use of This Flap
- •
Popliteal fossa
- •
Knee defects.
Postoperative Care and Expected Outcomes
General
See the Abductor digiti minimi (ADM) section.
Recipient Site
The operated side should be elevated and rested in a plaster splint.
Donor Site
The donor site is closed primarily if a fascia only flap was harvested. Standard postoperative occlusive dressings can be applied. If a skin graft was required, a negative-pressured vacuum dressing can be used as described previously.
Outcomes
Expected Outcomes
Temporary venous congestion or distal flap loss is often encountered. The major donor deficit of the flap is the loss of sensibility along the lateral aspect of the foot and a skin-grafted depression at the posterior calf donor site that may pose a problem if the patient later undergoes a below knee amputation. In a well-vascularized extremity, the pedicle can be removed after 3–4 weeks to improve the contour of the leg.
Untoward Outcomes
We have seen a near 40% complication rate, mostly due to venous congestion from a reverse sural flap. Risk factors for increased complications are older age; history of smoking; obesity; diabetes; and peripheral vascular disease.
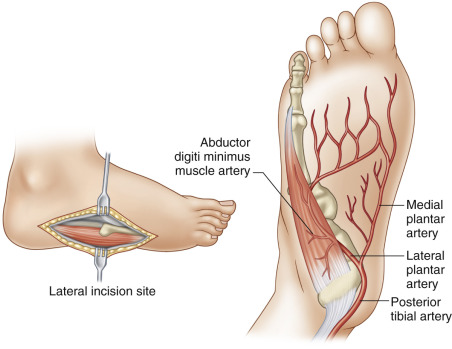
Abductor Digiti Minimi (ADM) Flap
The ADM (see Figs 13.11 and 13.16 ) is a triangular muscle with a wide posterior origin extending from the medial to the lateral process of the calcaneus, along with the adjacent intermuscular septum. The bulk of the muscle is found at the proximal portion of the 5th metatarsal. It ultimately inserts on the lateral side of the proximal phalanx of the small toe with the flexor digiti minimi brevis muscles. Anatomic variations can exist, with separate muscle bellies that stop and start at the opposite base of the 5th metatarsal. The muscle functions to abduct the small toe.
Flap Anatomy ( Fig 13.11 , Fig 13.16 , Fig 13.19 )
Arterial and Venous Supply of the Flap
Dominant:
one dominant pedicle from lateral plantar artery
Length: 2 cm
Diameter: 0.6 mm
Minor:
minor pedicle(s) from the lateral plantar artery (1–2)
Length: 1 cm
Diameter: 0.5 mm
ADM is a type II muscle with one dominant vascular pedicle and minor pedicles for its blood supply. The lateral plantar artery is responsible for both the dominant and minor pedicles to the flap. The major pedicle arises from the lateral plantar artery close to the origin of the muscle ( Fig. 48.3 ).
Venous Drainage of the Flap
Primary:
venae comitantes of the lateral plantar artery
Length: 1 cm (range 1–1.5 cm)
Secondary:
secondary venous systems are not significant.
Flap Innervation (see Fig 13.11 , Fig 13.19 )
Sensory:
branches of the sural nerve and lateral plantar nerves
A small skin paddle receives sensory innervations from the lateral plantar nerve, and the sural nerve can be included (not commonly used).
Motor:
branches of lateral plantar nerve
The ADM flap is not used as a motorized flap.
Flap Components
It is commonly taken as a muscle-only flap. Very rarely it is used as a musculocutaneus pedicled flap.
Advantages
- •
Ease with dissection
- •
Low donor site morbidities
Disadvantages
- •
Small size
- •
Small amount of distal tissue
- •
Short arc of rotation
Preoperative Preparation
As described previously, a complete understanding of the wound, a thorough history, and physical exam pertinent to wound healing should be undertaken. If the wound is infected, adequate surgical debridement needs to be done. All patients that undergo local muscle flap surgery require a thorough Doppler exam, with a complete understanding of the antegrade and retrograde components of the patient’s foot blood supply. If there is an abnormality, we recommend an angiogram or angiography prior to surgery. The lateral plantar artery coming off the posterior tibial artery must be patent. If the posterior tibial artery is not palpable over the tarsal tunnel, handheld Doppler or noninvasive vascular flow studies or angiography can be used for determining patency.
Flap Design
Anatomic Landmarks
Origin: lateral and medial processes of the calcaneus tuberosity and the intermuscular septum
Insertion: the lateral base of the 5th proximal phalanx
General Thoughts About Flap Design
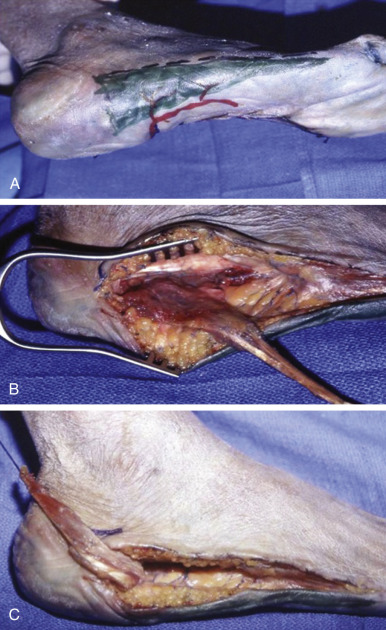
A line is drawn from the 5th metatarsal-phalangeal joint to the lateral heel along the glabrous junction between the dorsum and sole of the foot ( Figs 48.4 , 48.5A ). A Doppler probe is used to locate the major as well as the minor pedicles. Dissection should proceed from distal to proximal with loupe magnification, taking care to avoid injury to the muscle belly.

Special Considerations
Defects of the distal foot and 5th metatarsal joints can be covered by distally based ADM muscle. Dissection proceeds from proximal to distal, tying off the major pedicle as it enters the muscle medially. In our experience, basing this flap on the minor pedicles is unreliable.
Difference in Design, if Any, When Performing the Flap as Pedicled or Free
The ADM muscle flap is used as a local flap for reconstruction of the foot.
Flap Dimensions
Muscle Dimensions
Length: average 10 cm
Width: average 3 cm
Flap Markings
A line is drawn from the 5th metatarsal-phalangeal joint to the lateral heel along the glabrous junction between the dorsum and sole of the foot ( Fig. 48.4 ).
Patient Positioning
The patient is placed supine with a pillow for adequate exposure of lateral plantar surface of the foot. Careful attention to padding for any potential pressure points is essential.
Anesthetic Considerations
The ADM flap can be raised with regional block, especially in the setting of insensate neuropathic population. If an ankle block is to be used, 5 mL of 0.5% bupivacaine injected at the tarsal tunnel is required, with a wheel extending anteriorly around the ankle covering medial and lateral cutaneus branches of the superficial peroneal nerve and sural nerve.
Technique of Flap Harvest
A line is drawn from the 5th metatarsal-phalangeal joint to the lateral heel along the glabrous junction between the dorsum and sole of the foot. The incision is then made following the line drawn and taken down to the level of the muscle. The muscle is detached from the lateral 5th metatarsal-phalangeal joint by dividing the tendinous insertion. It is then elevated off of the flexor digiti minimi until one reaches the proximal portion of the 5th metatarsal. Once it has been divided from the insertion, a suture is placed in the distal tendon to allow manipulation and dissection with minimal trauma. The minor pedicles enter the muscle medially. The dominant pedicle is at the medial posterior corner of the cavity that houses the main bulk of the muscle belly and is derived from the lateral plantar neurovascular bundle ( Fig. 48.3 ). A Doppler probe is used throughout the case to mark the major as well as the minor pedicles. The origin of the muscle can be detached off of the lateral calcaneus for improved mobilization of the muscle. The muscle is inset using either PDS or Prolene suture. A split-thickness skin graft is subsequently harvested and secured on top of the muscle flap if necessary. The donor site can be closed primarily ( Fig. 48.5 ).
Flap Modification/Flap Handling
The ADM muscle flap can be used in conjunction with other intrinsic muscle flaps of the foot for coverage of larger defects. ADM can be used with abductor hallucis brevis to cover a larger plantar heel defect. ADM can be used with extensor digitorum brevis for the coverage of lateral malleolar soft tissue defects.
Special Instruments
A handheld Doppler should be readily available. A dermatome can be used for the harvesting of the skin graft.
Donor Site Closure and Management
Donor site can be closed primarily when a muscle-only flap is harvested. With a musculocutaneous flap, a split-thickness skin graft will likely be needed to close the donor defect.
Technical Tips to Optimize Outcomes and Avoid Complications
- •
Avoid tension near the posterior aspect of flexor digitorum brevis (FDB), where the pedicle will rotate.
- •
Distal elevation of adherent attachment to the base of the 5th metatarsal bone requires care.
Flap Usage
Pedicled
The muscle has a small arc of rotation. It will cover small defects on the distal lateral ankle, distal Achilles tendon, and distal fibula.
Typical Indications for the Use of This Flap.
The ADM muscle is very useful in repairing small lateral calcaneal soft tissue defects.
Atypical Indications for the Use of This Flap.
It can also be used for larger plantar heel defects, when used in conjunction with either or both the flexor digiti brevis and the AHB muscle. Further modifications have expanded the indications to toe reconstruction when it is raised distally.
Postoperative Care and Expected Outcomes
General
A standard postoperative care includes pain control and management of medical commodities, such as an aggressive glucose management for diabetics. Perioperative antibiotics, culture-directed when possible, should be used following the procedure.
Recipient Site
A bolster dressing or a vacuum-assisted negative-pressure wound therapy can be used for the first 3–5 postoperative days to assist in the skin graft taken. The ankle joint should be immobilized in a neutral position to avoid tension at the suture line. The patient will need protection of the flap with a splint, a Cam walker boot, or a cast at discharge until the first postoperative visit. Patients are typically non-weightbearing for 4 weeks postoperatively.
Donor Site
The donor site is often closely primarily. Standard postoperative occlusive dressings can be used for the first 2 days after the procedure.
Outcomes
Expected Outcomes
With adequate flap protection, we expect the flap to survive. Based on our experience, the flap has at least a 96% success rate in the diabetic and non-diabetic population, which is comparable with microsurgical reconstruction in a similar population.
Untoward Outcomes
Without adequate blood glucose control and management of comorbidities, and avoidance of vasoconstrictive substances (tobacco), patients can develop total or partial flap loss.
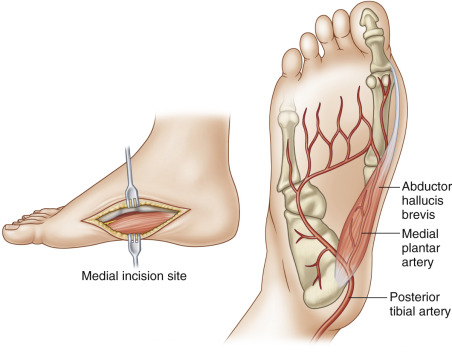
Abductor Hallucis (AH) Flap
The abductor hallucis (AH) muscle is located in the medial plantar region between the great toe and the base of the heel. The muscle arises from the calcaneus medially with a wide muscle belly, and then tapers into a long tendinous insertion to the great toe. The muscle is expendable and functions to abduct the great toe.
Flap Anatomy (see Fig. 48.6 and Fig 13.11 , Fig 13.19 )
Arterial and Venous Supply of the Flap
Dominant:
proximal branch of medial plantar artery
Length: 2 cm
Diameter: 0.6 mm
Minor:
minor branches of medial plantar artery (2–3 branches)
Length: 1.5 cm
Diameter: 0.5 mm
The medial plantar artery courses between the AH muscle and flexor digitorum brevis and flexor hallucis brevis muscles. AH is a type II muscle with one proximal dominant pedicle and 2–3 minor pedicles ( Fig. 48.6 ).