CHAPTER 38 Local Flaps for Tuberous and Asymmetric Breasts
Key Points
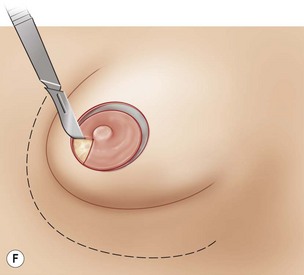
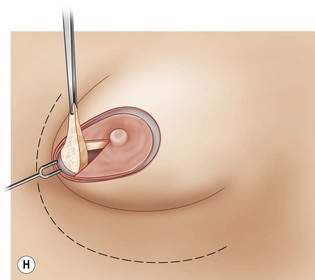
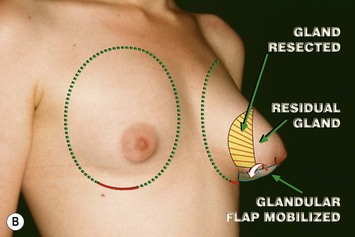
4. Type I is an inferior glandular flap that is turned down beneath the gland toward and secured at the IMF.
5. Type II is an inferior glandular flap that is turned down beneath the gland to fill out the constricted lower pole.
6. Type III is an inferior glandular flap that is reversed and used beneath the skin to fill out more superficial constrictions.
7. Often breast asymmetry is best treated by removing parenchyma in the larger breast, using appropriate flaps as described and then using similar sized implants.
Summary
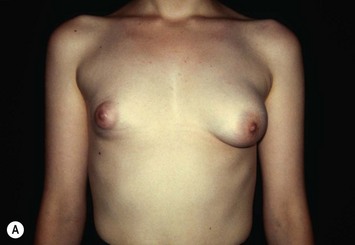
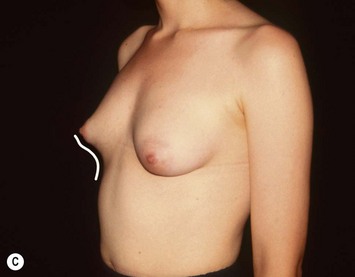
In this chapter I will consider only the ‘heavily hypoplastic tuberous breast.’
Many surgical techniques have been described to best treat these malformations1–20 but none of them, in my opinion, seem to be perfectly applicable to each case and to each different morphological anomaly.
I have developed a new ‘basic idea’ which can be tailored to fit each clinical case.
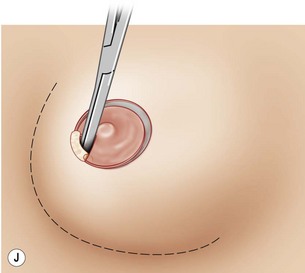
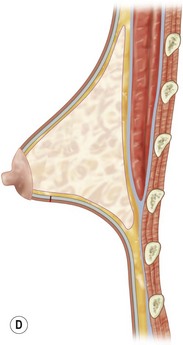
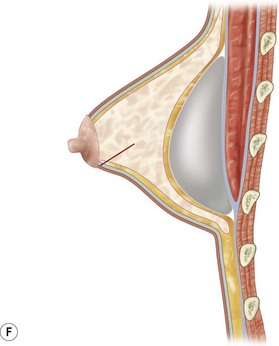
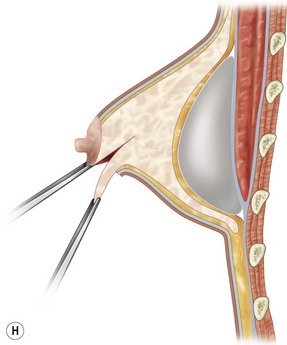
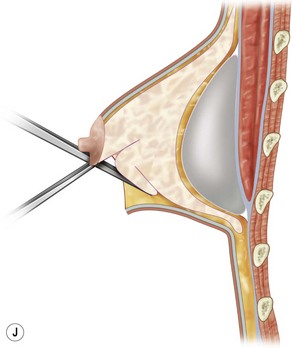
The flaps need to be long enough to reach the pectoralis muscles once the fibrotic constriction of the breast base is released. This constriction often needs to be released by radial and transverse incisions from the deep surface as described by Aston and Rees,14 and Maxwell.9
Patient Selection and Indications
• Each single flap, described above, can be utilized for selected patients who present different and specific morphological characteristics.
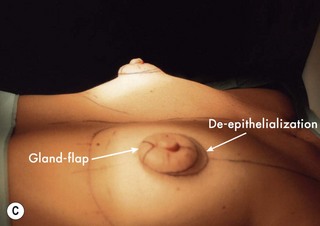
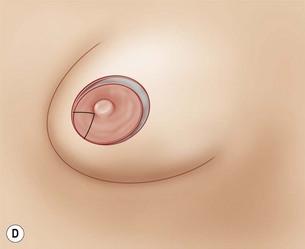
• Flap Type I (Figs 38.3–38.16) and flap Type II (Figs 38.28–38.35) are indicated in cases of minor or major evidence of herniation of the gland into the areolar skin respectively.
• Flap Type III is usually combined with some release incisions of the gland and is indicated in cases with tight, tense and more or less concave inferior pole without defined inframammary fold (Figs 38.46–38.53).