Otoplasty can be performed safely and effectively under local anesthesia in children as young as 5 years of age. Child preparation, local anesthetics, detailed infiltration technique, surgical procedure, and complications are discussed.
Key points
- •
Children as young as 5 years old can be operated safely under local anesthesia, without premedication or sedation.
- •
Local anesthetics, either short-acting or a combination of short-acting and long-acting, with adrenalin are used with a very slow infiltration rate.
- •
Constant attention is directed to the child to explain the procedure and reduce the level of anxiety.
- •
The anesthesia obtained is appropriate for different otoplasty techniques, either suture-correction or anterior scoring.
- •
Appropriate doses of local anesthetics in relation to the child’s weight and possible complications are reviewed.
- •
The surgical complications do not differ from surgeries performed under general anesthesia.
Otoplasty is a procedure that can safely and efficiently be performed under local anesthesia in children. Making the decision to undertake the procedure under local rather than general anesthesia is first the surgeon’s choice and then the child’s and child’s parents. The surgeon must be intimately familiar with the surgery because his attention will be partially diverted to chat with the child and reassure him during the procedure. Furthermore, the duration of the procedure should not be excessive because the child becomes restless after 50 to 60 minutes.
Two factors are helpful when performing local anesthesia on the ear:
- 1.
The discrimination of the ear for pain perception is not as good as other areas of the body, such as the nose, the lips, or the fingers.
- 2.
The location of the ear makes it impossible for the child to see what is happening; thus, it is easier to reassure him.
Patient selection
Deciding which patient is well suited to have the procedure under local anesthesia depends mainly on the opinion of the child concerning his ears and his motivation for a correction. Placing the child in front of a mirror during the first consultation to show him the change that can be achieved in the shape of his ears is helpful to let him decide whether he likes the new ear shape or not. A child who does not want to change his ears will certainly not accept local anesthesia. The family can then decide to proceed under general anesthesia or wait for the child’s collaboration to have the procedure under local anesthesia.
When the child is motivated to have the surgery, the procedure is explained in simple terms avoiding the words “needle” and “cut” but rather “putting the ear to sleep with a pinch,” “folding the ear cartilage,” and “placing a dressing” for a week. It is important to obtain the child’s approval for the plan, insisting on the fact that the only reason to change the ear shape is to please him.
The parents are sometimes surprised with this attitude and the fact that the decision is left to the child, but the majority see this very positively. The parents are asked not to add more details about the anesthesia or the surgery but rather repeat the same explanations. In my practice, more than 95% of otoplasty in children age 5 and older are performed under local anesthesia. The referring physicians are well aware of it and often have informed the parents so it is unusual for a family to refuse local anesthesia. If, for any reason, a family did refuse, one should not impose local anesthesia.
Patient preparation
The child is not admitted to the hospital for the surgery; he comes to the outpatient clinic where the operating room for local anesthesia is located. His parents have been asked to wash the child’s hair the same day or the day before and to feed him normally. No premedication is used; it is easier to control a child who is not sedated and can answer questions, play with words, and keep his mind busy. Topical anesthetic cream before the infiltration is not used routinely: the skin puncture with a 30-gauge needle is not easily detectable by the child. The pain due to tissue distension from the infiltration is unchanged with a topical anesthetic. However, if the family thinks that it is helpful, the author lets them apply the cream 60 minutes before the procedure on the posterior surface of the ear only.
- •
The child is brought in the operating room ( Fig. 1 A) only when the instruments and the syringe are prepared and covered (see Fig. 1 B) and the surgeon is ready.
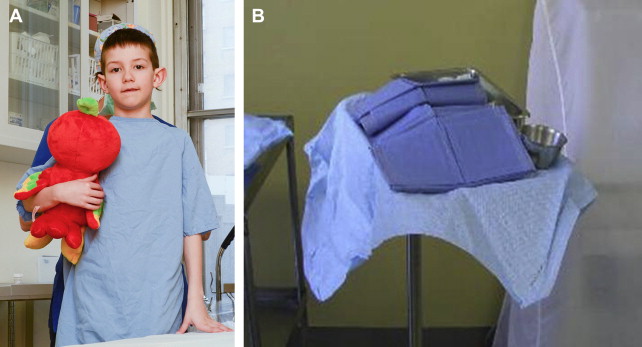
Fig. 1
( A ) Child walking in the operating room without his parents. ( B ) Instruments and syringe hidden.
- •
The parents are asked to sit in a waiting area adjacent to the operating room; it is easier for the surgeon to focus his attention on the child and maintain a one-on-one conversation.
- •
There is no intravenous or monitoring equipment installed and the child is not restrained; he is simply asked to lie on his back with his hands hidden behind his back ( Fig. 2 ). No antibiotics are used.

Fig. 2
Child lying down unrestrained hiding his hands behind his back.
- •
The face, ears, and peri-auricular areas are cleansed with aqueous chlorhexidine solution and a head drape is used, keeping the face completely exposed.
Anesthesia administration note : The author insists on a calm, reassuring, and friendly environment, low voices, no conversation except with the child to explain what is happening and what he may feel. It is important to make the child understand that he is in control: he uses a simple word “gentle” to slow down the infiltration and control the pain. The infiltration is stopped as soon as the child asks for it. He quickly understands his “power” and becomes more tolerant knowing that he can stop the pain anytime: it is a “patient-controlled anesthesia.”
- •
The duration of the procedure including the local anesthesia, the surgery, and the dressing is 1 hour, which is well tolerated by the children.
Patient preparation
The child is not admitted to the hospital for the surgery; he comes to the outpatient clinic where the operating room for local anesthesia is located. His parents have been asked to wash the child’s hair the same day or the day before and to feed him normally. No premedication is used; it is easier to control a child who is not sedated and can answer questions, play with words, and keep his mind busy. Topical anesthetic cream before the infiltration is not used routinely: the skin puncture with a 30-gauge needle is not easily detectable by the child. The pain due to tissue distension from the infiltration is unchanged with a topical anesthetic. However, if the family thinks that it is helpful, the author lets them apply the cream 60 minutes before the procedure on the posterior surface of the ear only.
- •
The child is brought in the operating room ( Fig. 1 A) only when the instruments and the syringe are prepared and covered (see Fig. 1 B) and the surgeon is ready.
Fig. 1
( A ) Child walking in the operating room without his parents. ( B ) Instruments and syringe hidden.
- •
The parents are asked to sit in a waiting area adjacent to the operating room; it is easier for the surgeon to focus his attention on the child and maintain a one-on-one conversation.
- •
There is no intravenous or monitoring equipment installed and the child is not restrained; he is simply asked to lie on his back with his hands hidden behind his back ( Fig. 2 ). No antibiotics are used.
Fig. 2
Child lying down unrestrained hiding his hands behind his back.
- •
The face, ears, and peri-auricular areas are cleansed with aqueous chlorhexidine solution and a head drape is used, keeping the face completely exposed.
Anesthesia administration note : The author insists on a calm, reassuring, and friendly environment, low voices, no conversation except with the child to explain what is happening and what he may feel. It is important to make the child understand that he is in control: he uses a simple word “gentle” to slow down the infiltration and control the pain. The infiltration is stopped as soon as the child asks for it. He quickly understands his “power” and becomes more tolerant knowing that he can stop the pain anytime: it is a “patient-controlled anesthesia.”
- •
The duration of the procedure including the local anesthesia, the surgery, and the dressing is 1 hour, which is well tolerated by the children.
Local anesthesia technique
The ear is vascularized by branches of the external carotid artery via the superficial temporal and the posterior auricular arteries. The innervation is provided by the greater auricular nerve (anterior and posterior branches) for the lower anterior and posterior regions including the lobule, branches of the auriculotemporal nerve for the anterior upper surface and branches of the lesser occipital nerve for the upper posterior surface. This anatomy makes it less favorable for regional nerve blocks; therefore, local anesthesia infiltration is performed directly in the auricle. This direct infiltration also provides hydrodissection and vasoconstriction of the region. It is well adapted to the anterior scoring technique with direct exposure of the cartilage, or a suture technique.
- •
The author routinely uses 1% lidocaine with 1/100,000 epinephrine; a total volume of 10 ml or less is used for both ears.
- •
The infiltration begins with a 30-gauge needle in the subcutaneous tissue on the posterior surface of the ear, where the skin is less adherent to cartilage and more easily distended.
- •
Pinching the ear very close to the site of needle puncture ( Fig. 3 ) distracts the child’s attention from the needle.
Fig. 3
The ear pinched between 2 fingers adjacent to the 30-gauge needle puncture.
- •
Only a small volume of fluid is infiltrated when the needle is advanced under the skin ( Fig. 4 ); more volume is injected as the needle is withdrawn.






