Fig. 48.1
First step in controlling liver bleeding: completely mobilize the liver from the diaphragm
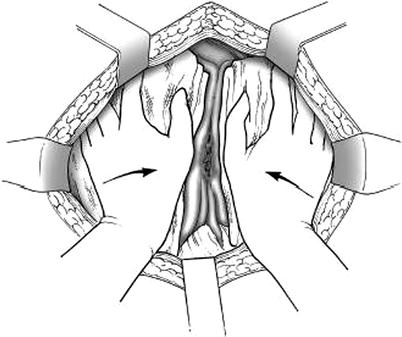
Fig. 48.2
Second step in controlling liver bleeding: manual compression with hands compressing both lobes toward the hepatic hilum
The next key step is to distinguish between arterial and venous injury. An insightful surgical aphorism states: “Arterial bleeding scares the amateurs, venous bleeding scares the professionals.” The Pringle maneuver is useful to distinguish amateur from professional bleeding from a penetrating liver injury. One can accomplish it in a matter of seconds by passing your left index finger through the foramen of Winslow and directing it anteriorly through the lesser omentum (gastrohepatic ligament). This is done bluntly. Once the fingertip appears, sweep a three-quarter-inch Penrose drain around the porta hepatis in the same manner one encircles the spermatic cord during a hernia repair. The Penrose can then be tightened with a Kelly clamp to occlude all inflow to the liver (Fig. 48.3a, b). The time inflow occlusion starts should be recorded. Ideally, hepatic ischemia should be limited to 30 min or less. If this arrests the bleeding, then arterial hemorrhage is almost always the problem. If bleeding persists, then injury to a hepatic vein or adjacent vena cava should be suspected.
Fig. 48.3
(a) Pringle maneuver step A: insert left index finger into the foramen of Winslow, and then push the finger tip through the lesser omentum (aka gastrohepatic ligament). (b) Pringle maneuver step B: encircle the porta hepatis with a ¾″ Penrose drain hooked around the index finger, then tourniquet the porta by twisting the drain and securing with a Kelly clamp
In the case of brisk arterial bleeding, threatening immediate exsanguination, ligation of the common hepatic artery or the right or left hepatic artery is an alternative. With the Penrose drain–Pringle tourniquet on downward traction, you can find the hepatic artery by first identifying the common bile duct and looking medially.
Prior to closing the abdomen with towel clips, packs are applied anteriorly across the surface of the liver. If you have ligated or embolized the right hepatic artery, the gallbladder will be devascularized and should be removed.
If the Pringle maneuver does not arrest the bleeding, then assume venous injury. At this point, it is important to evaluate the vena cava for injury. Many times the real source from liver injuries is in fact the vena cava or the junction of the vena cava and hepatic veins. Vena caval injuries can be classified into three types: suprahepatic, retrohepatic, and infrahepatic.
If a suprahepatic injury is suspected, proceed directly to a thoracoabdominal approach. While a “hockey-stick” incision into the costal cartilages from the superior pole of the midline wound is possible, I prefer to perform median sternotomy in cases where injury to the cava appears to be in the “no man’s land” between the liver and heart. These wounds have a very high mortality. Successful management requires rapid control which is best gained by dividing the sternum and diaphragm. The sternum is best divided with a power-driven sternal saw. Finger dissection in the suprasternal notch to keep the innominate veins away from the saw blade is a good first step. Next, with the saw guard introduced through the sternal notch and on upward traction, the sternum can be opened in a matter of seconds. A Finochietto retractor or similar rib spreader can provide access to the heart and mediastinum. Take down the pericardium and anterior attachments of the mediastinum quickly with scissors. Divide the diaphragm with the cautery down onto the caval hiatus. This should expose the injured segment. A side biting vascular clamp is usually the simplest tool for controlling the injury. Once the clamp is on, blood return to the heart will be minimal. Mortality for these injuries is very high. It is essential that one work with alacrity in the setting.
Retrohepatic caval injuries are among the most challenging injuries the trauma surgeon faces. In the setting of penetrating trauma, where bleeding is not contained within a soft tissue space, the vena cava must be exposed rapidly. In patients where the liver is relatively large or this exposure is difficult, access to the chest as described above may be useful. Generally, however, it is not necessary to open the chest to approach the retrohepatic vena cava. Having already mobilized the ligamentous attachments, it is possible to rotate the liver medially exposing the retrohepatic cava. If the injury involves the intrahepatic portion of the cava, it may be necessary to take down the small veins draining directly from the substance of the liver into the vena cava. These usually number between 7 and 14 and in an emergency can be well managed with small clips. Failure to control these veins will result in the creation of an additional source of bleeding. Inflow and outflow occlusion of the cava above and below the injury can be usually achieved with direct compression using sponge sticks. As in the suprahepatic vena cava injury, there is a high premium on efficiency. Having 3-0 or 4-0 vascular nylon suture ready on a long needle driver prior to diving in to the retrohepatic space is a good idea.
Injuries to the infrahepatic cava can be exposed by the so-called Braasch–Cattell maneuver, where one opens the white line of Toldt in the right paracolic gutter and sweep the right colon medially on its mesentery. Mobilize the duodenum medially in a similar way. Sponge sticks are useful here too for proximal and distal control in a hurry. Traditionally, it has been thought that it is necessary to preserve at least 25 % of the lumen of the vena cava above the kidneys. Recent experience indicates less lumen may be acceptable, it is certainly better to leave a conduit of diminished diameter than ligate the cava or, worse, have a patient expire while performing an interposition graft. Endovascular stenting is emerging as an option for the management of penetrating injuries of the infrahepatic vena cava.
Where patients are unstable and complex injury of the infrahepatic vena cava precludes a simple vascular repair, ligation is an acceptable option, though mortality in cases requiring IVC ligation exceeds 50 %.
Patient suffering from multiple gunshot wounds to the liver or injuries caused by high-velocity rounds or military ordinance may have complex, massive, liver fractures, difficult to control by packing. These wounds are fortunately rare in civilian practice. Bleeding uncontrollable by packing disqualifies the patient for a damage control procedure. It is in this setting that maneuvers such as hepatic exclusion may be the only option. With the Pringle tourniquet engaged, the hepatic inflow and outflow controlled with sponge sticks, one looks for the dominant sources of hemorrhage and clips or ligates them. In limited cases, formal lobectomy may be preferable if the injury is limited to an anatomic lobe or segment.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


