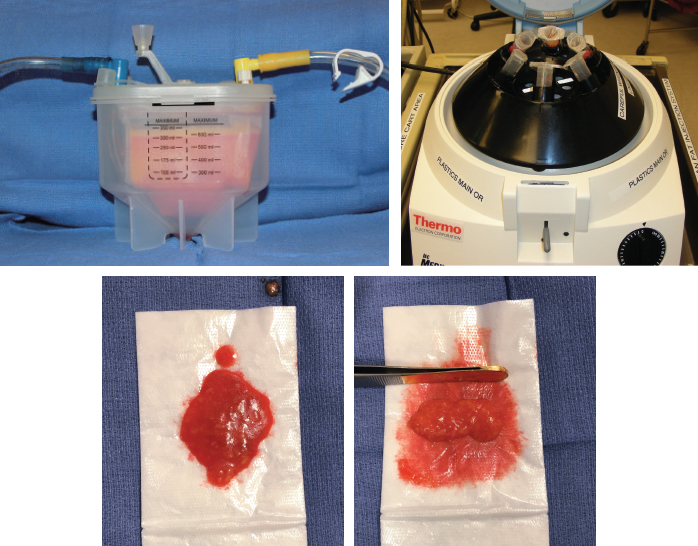
CHAPTER 16 Kamran Khoobehi Fat grafting became popular in the 1980s with the advent of liposuction. Before this time, fat grafting was not widely accepted because of its unpredictable results and high failure rates. Czerny in 1895 first reported using autologous fat transplantation to contour a breast defect. Interest in fat grafting was renewed with the introduction of liposuction by Illouz. Fat grafting techniques have recently become part of residency education, and fat grafting is consistently a hot topic at major national meetings. However, there still exists a large variation from surgeon to surgeon on techniques for harvesting, processing, and injecting fat, which has led to some unpredictable outcomes and results. Currently, there is no published consensus on the optimal techniques for autologous fat grafting, which leads to both patient and surgeon frustration. In this chapter we will outline the principles of fat grafting as well as our techniques, with a goal of helping surgeons to attain more predictable results and satisfaction with fat grafting. Several different processing methods exist currently, so it can be difficult for surgeons to select an optimal method when beginning to incorporate fat grafting in their practice. Centrifugation, gravity separation, filtration, and gauze rolling are all techniques currently used to process the harvested fat. Stromal vascular fraction (SVF) cells and adipose-derived stem cells (ADSCs) have been shown in multiple studies to enhance the survival of grafted fat, mainly by inducing angiogenesis. Therefore determining an ideal processing method would increase the number of SVF cells and ADSCs in the fat, enhancing the final result. The ideal method must also be efficient for both low-volume and high-volume fat grafting to decrease overall operative time. Recently, the gauze rolling method has been shown to increase the number of viable cells and ultimately the volume of fat retention when compared with other methods. However, this method may not be efficient for large-volume fat grafting for body contouring. Despite the numerous studies in the literature, there is still not a consensus on the perfect processing method. When all studies are evaluated, it is clear that one process cannot be declared superior to the others at this time. Fig. 16-1 Several of the current processing methods include the REVOLVE Fat Grafting System, the Body-Jet LipoCollector, centrifugation, and gauze rolling. With the low-pressure liposuction technique, liposuction both superficial and deep to the Scarpa layer can be performed at the donor sites to provide the optimal contour without increasing the risk of contour deformities. For the breasts, multiple anatomic layers are injected to create an aesthetic contour. Fat is grafted to the submuscular and subglandular spaces to provide added projection to the breasts. Intramuscular injection is avoided, because this may lead to calcifications that are visible on mammograms. Grafting to the subcutaneous space creates cleavage and a smooth contour to the breast. ■ It is essential to inject the fat only while withdrawing the cannula. ■ Special attention should be given to the medial quadrant of the breast, where large intercostal perforators exist. ■ When injecting the submuscular space, the cannula should always be parallel to the chest wall to avoid inadvertent entry into the thoracic cavity. ■ With the use of a blunt cannula and injecting on withdrawal, the risks of fat emboli and nerve injuries are reduced, and occur rarely. The physiologic considerations associated with liposculpture are from the potential fluid shifts that can occur with large-volume liposuction. We recommend for outpatient procedures that the total volume of lipoaspirate be limited to 5 L to avoid potential complications. If a larger volume is suctioned in a single procedure, the patient should remain in the hospital overnight for close monitoring of fluid resuscitation. An ideal patient for liposculpture plans to avoid extreme weight fluctuations after surgery. Postoperative results can be jeopardized if a patient either gains or loses a large amount of weight after fat grafting. The patient must be healthy and not possess any comorbidity that would preclude him or her from undergoing a cosmetic or reconstructive procedure. Virtually every part of the body can undergo liposculpture and fat grafting, and the indications are broad. Fat grafting can be added to almost every cosmetic and reconstructive procedure to enhance the postoperative result. We commonly use fat grafting in breast reconstruction, for breast augmentation with and without implants, with mastopexy, and for patients who have had severe complications with implants. Patients who request breast augmentation of more than one cup size are not great candidates for pure breast augmentation with fat grafting; such patients are usually better suited for breast implants or will require repeated breast fat grafting procedures to achieve more than one cup size larger. Patients who have complications from liposuction can also benefit from filling contour deformities with fat grafting. Augmentation of the hips with fat during abdominoplasty and buttock augmentation with fat are also very common in our practice. Before embarking on liposculpture, a plastic surgeon must pay careful attention to the potential donor sites. As plastic surgeons, our duty is to not only improve the recipient site but also to avoid leaving the donor site with a deformity. Therefore both the donor and recipient sites are of equal importance. Any previous liposuction procedures must be noted, because repeat liposuction in the same donor site can increase the risk for potential complications. A question that must be asked is whether the patient has enough fat to harvest for a certain fat grafting procedure. Although some body builders or athletic patients certainly are not candidates for fat grafting procedures, it is beneficial to pay close attention to the thighs in thin female patients. A quick examination of the thighs or even other body areas can help the surgeon decide whether there is enough fat to harvest for a certain procedure.
Liposculpture: Fat Injection Techniques in the Body
 Jules A. Walters III
Jules A. Walters III
Surgical Anatomy
Physiologic Considerations
Indications and Contraindications
Patient Evaluation
CLINICAL EVALUATION OF THE DONOR SITE
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine