Brian P. Maloney, William Truswell IV, and S. Randolph Waldman, address questions for discussion and debate:
- 1.
Is surgery ever a better alternative than injectable fillers for enhancement of the lips?
- 2.
What role do permanent lip implants play for today’s patients?
- 3.
How do you manage the small-mouthed person seeking lip enlargement?
- 4.
How do you handle down-turning corners of the mouth?
- 5.
How do you handle a person who previously had full lips but now is losing volume, especially in the corners?
- 6.
What qualities of the lip are important to preserve when considering various lip augmentation materials and techniques?
- 7.
What are the best ways of reducing the length of the upper lip?
- 8.
Analysis: Over the past 5 years, how has your technique or approach to lips changed, or what is the most important thing you have learned in performing lip augmentations?
Brian P. Maloney, William Truswell IV, and S. Randolph Waldman, address questions for discussion and debate:
- 1.
Is surgery ever a better alternative than injectable fillers for enhancement of the lips?
- 2.
What role do permanent lip implants play for today’s patients?
- 3.
How do you manage the small-mouthed person seeking lip enlargement?
- 4.
How do you handle down-turning corners of the mouth?
- 5.
- 6.
- 7.
What are the best ways of reducing the length of the upper lip?
- 8.
Video of surgical technique of subnasal lip lift and advancement of lower lip accompanies this article. Available at : http://www.facialplastic.theclinics.com/
Is surgery ever a better alternative than injectable fillers for enhancement of the lips?
Maloney
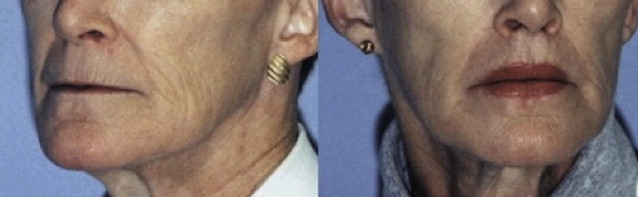
Yes, surgery may be a better alternative for the patient with thin lips and poor definition of Cupid’s bow. For the patient with congenitally thin lips, the vermilion advancement is an excellent means of increasing the amount of vermilion show. This procedure can be combined with lip augmentation procedures if additional bulk is desired ( Fig. 1 ).

Surgery is also an excellent procedure for the patient who desires lip augmentation; however, the upper lip may be too long and the patient may display no incisor show. Augmenting the lips in this case would only make the lip longer, throwing the lips more out of balance. A nasal-base resection would be a better alternative to augmentation. Once the length of the lip is shortened, augmentation can be performed if necessary.
Acellular human dermal matrix graft augmentation of the lips can be an excellent means of creating more vermilion show in a thin-lipped patient. This surgical procedure is performed through a single incision in each commissure; a submucosal tunnel is created, and the matrix can be placed into both upper and lower lips.
When cosmetic surgeons attempt to create large lips from small ones by injecting fillers, the end result is generally a duck-bill, stiff, sausage-like look to the lip. The most commonly used lip fillers are hyaluronic acid fillers. By their physical nature they are liquids. Liquids by definition take the shape of their containers. It is very difficult to stretch a vermilion with a liquid filler and have it result in a natural long-lasting change. With increasing refinements of hyaluronic acid, newer products offer a higher degree of cohesiveness. Cohesiveness refers to the molecules’ ability to stay together and resist being dispersed. For high-motion areas that require augmentation, these highly cohesive fillers will offer more semisolid properties; however, the end result of overfilling with the latest fillers generally is an overdramatic feature.
I have found multiple V-Y advancements of the entire wet lip surface as an augmentation technique to result in a bulky lip with poor movement. Lips are very dynamic in nature, and any surgical procedure needs to maintain a soft flexible lip to allow it to function properly. Man-made implants such as those using expanded polytetrafluoroethylene (ePTFE) and saline as fillers, tend in my experience to restrict lip movements and often result in extrusion when placed in the upper lip. The lower lip is more tolerant of the implants because of its more basic structure and movement.
Truswell
Surgical lip enlargement should be considered in patients with very thin lips for whom injectable fillers or implants would be more distorting than enhancing. The best way to help these patients, in my opinion, is to perform a direct lip lift, a subnasal lip lift, or a V-Y augmentation. All of these procedures have varying results and can be fraught with complications.
Direct lip lifting is performed by excising a portion of the white lip and advancing the mucosa upward as an advancement flap. This technique will shorten the white upper lip. The incision should be placed above the white roll of the upper lip to preserve this feature. Meticulous closure is paramount in minimizing the scar that will occur. The patient must understand this issue. The scar can be camouflaged with dermabrasion or laser resurfacing. Lipstick can hide it, as can cosmetic tattoo. If not done with skill and precision, the scar can be emotionally and socially debilitating ( Figs. 2 and 3 ).