Key points
- •
The relevant surgical anatomy of the midface and eyelid are demonstrated to show the safest plane of dissection.
- •
The zygomaxillary anthropometric point is a key anthropometric structure in the creation of an aesthetically pleasing cheek mound.
- •
The differentiation of aesthetic cheek configuration complex in a male and female.
- •
Methods to efface the tear trough deformity.
- •
The role of the Bichat’s fat pad and other structures in creating the ‘ogee line’ of the midface.
- •
Prevention of complications.
Introduction
Despite the numerous techniques described over the decades, the midface has been one of the areas of the face resilient to standard-open or semi-open methods of treatment. Paradoxically, despite the minimal incision for access, the midface has been more amenable to the endoscopic techniques because it is possible to approach the deep layers of the midface directly at the safest plane of dissection. This allows for significant soft tissue remodeling.
Patient selection
All patients, whether young, middle-aged or elderly, are candidates for midface rejuvenation with minimal incisions. It is equally applicable to male and female patients and can be done on those with excellent as well as poor skeletal support. In young and very young individuals, I apply the principles of three-dimensional facial rejuvenation of the midface for purposes of enhancement. For strategic and conceptual reasons we do not call it facial rejuvenation but instead use the term ‘facial beautification’. I have performed these procedures to lift and reshape the face for aesthetic purposes in individuals as young as 18 years old.
When a man or woman starts developing the first signs of aging in their middle 30s, these usually manifest as the development of early tear trough deformity, sagging of the cheeks and presence of nasolabial folds. These are the group of patients that can benefit the most from endoscopic minimal incision midface rejuvenation. This is because the changes with facial rejuvenation are not quite as dramatic as in older individuals. Even in those with more dramatic changes, the procedure produces natural results with a lack of telltale signs of surgery which are particularly welcomed by patients who want to return to normal activities as quickly as possible.
Middle-aged, late middle-aged and elderly individuals are also excellent candidates for the procedure because the endoscopic midface lift can be easily incorporated as part of a more extensive and complete facial rejuvenation. In fact, I use basically the same midface lift technique for all ages and for all individuals. For those requiring more volume augmentation or correction of soft tissue asymmetries, I add fat grafting techniques. For those requiring skeletal augmentation in the pyriformis, malar or orbital areas I use the corresponding facial implants during the endoscopic minimal incision midface lift. Men are equally good candidates for the procedure. The only difference from their female counterparts is that the final aesthetic shape of the cheek is slightly different. This will be elaborated on later in the chapter.
Indications
Patients with early or considerable aging or ptosis of the structures of the central oval of the face can benefit from the endoscopic minimal incision midface lift. Eyelid commissure, nasolabial folds, cheeks, angle of the mouth are effectively treated with this approach. Moderate tear trough deformities and infraorbital hollows are also correctible with endoscopic techniques. The endoscopic midface procedure allows for recreation of the ogee of the midface. This reciprocal multi-curvilinear line is associated with a youthful and beautiful appearance. The endoscopic minimal incision midface lift is also quite effective for patients requiring secondary or tertiary face lift procedures, for those patients requiring deep chemical peel or CO 2 laser resurfacing, and for patients requiring soft tissue augmentation via fat grafting. In the first case dissection of the midface is performed in areas previously untouched by prior procedures. Dissection is, therefore, done in a virgin subperiosteal plane. In the second case, the composite thick flaps have excellent vascularity and ablative procedures performed on the skin do not affect its survival. In the last case, the intermediate and superficial lamellae of the face are intact and fat can be injected in as many multiple tunnels as needed.
Patients with skeletal or soft tissue disproportion can also benefit from endoscopic techniques of the midface. The exposed bony structures can be augmented via implants or reduced by osteotomies or bone burring without the need to go to a different plane of dissection as is the case when surgery is performed in the superficial or the intermediate plane of the face.
Pre-operative preparation
A full medical history including cardiac clearance is required. In this age of significant influence by fashion and the media, patients will do anything to maintain their slim figures including adhering to a restrictive diet. For this reason, many young patients present to their plastic surgeon with an undiagnosed or untreated case of anorexia and/or bulimia. These patients, despite their deceptively normal appearance may be in severe metabolic and electrolyte deficit and imbalance which may include hypokalemia and hypomagnesemia. These disorders can lead to an unexpected cardiac arrest during or after surgery, among other complications. Surgeons, particularly plastic surgeons, should be aware of this potential situation.
Photographs with minimal or no makeup are taken several days before surgery. Hair is pulled back from the face with hairbands, clips and elastic bands. No tension of the brows or temples should be made with these in order to prevent ‘photo-surgery’. The ears, temples, forehead and neck should be fully exposed in the photographs. For photographs of the neck, a low-cut V or circular shirt or T-shirt should be worn by the patient ( Figure 12.1 ).

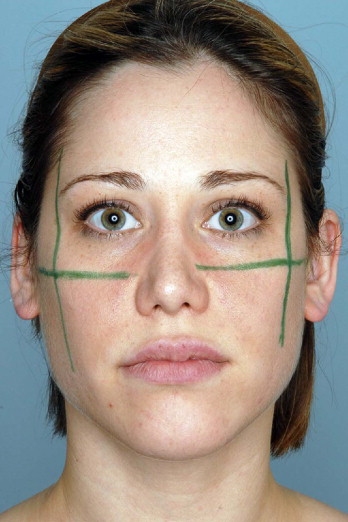
Markings are done with the patient in a standing or sitting position. The orbital rim outline is marked in blue. The area of maximal midface projection which is at the zygomaxillary point is marked in green. The nasolabial fold and tear trough deformities are marked in red as well as other areas of contour deficit. Areas of contour excess are marked in black. The jaw line and the cervicomental break are marked in blue ( Figure 12.2 ).

The patient is positioned supine but the operative table should have a tilt mode to move the patient 30–45 degrees sideways to prevent forceful twisting of the neck for exposure. Infiltration of local anesthetic/ vaso-constrictive agents used for the temporal and midface are a mixture of 0.5% xylocaine with 1 : 200 000 epinephrine solution. Approximately 30 ml of this solution is injected per site to the midface and temporal areas. The infiltration is done in titrated amounts and I use a blunt cannula of 0.9–1.2 mm outer diameter (Tulip Medical, San Diego, CA) after a puncture wound of about 1 mm is done with a #18 gauge Nokor needle. This blunt infiltration prevents micro-hematomas which are usually seen with sharp needles and also prevents inadvertent intravascular injections.
Technique
To aid in the description of the surgical technique the anatomical nomenclature used is outlined in Table 12.1 . The goal of the surgical procedure is to correct the tear trough deformity, lift the cheek, efface the nasolabial fold, enhance the projection of the cheek, and lift the corner of the mouth. Most important is the recreation of the youthful appearance of the cheek mound. The cheek seen in a three-quarter view has a specific outline that has the shape of sigma or Greek S, also called the ‘ogee line’ ( Figure 12.3 ). This starts with a slight concavity on the lateral orbital area gradually changing to a significant convexity of the cheek. This convexity gradually goes down at the level of the upper lip to converge into a slight concavity lateral to the para-comissural area. The highest point of the cheek convexity seen in a three quarter view is located at the so-called ‘zygomaxillary point’. This is a new anthropometric soft tissue point that can be located by the intersection of two lines: one traced vertically on the lateral external orbital rim and another line horizontally oriented extending from the upper lateral cartilage of the nose to the tragus ( Figure 12.4 ).
| Initials | Author’s preferred name | Other name |
|---|---|---|
| TLF | Temporal line of fusion | None |
| STF | Superficial temporal fascia | Temporo-parietal fascia |
| TFP | Temporal fascia proper | Temporalis fascia Deep temporal fascia |
| ITF | Intermediate temporal fascia | Superficial layer of the deep temporal fascia |
| DTF | Deep temporal fascia | Deep layer of the deep temporal fascia |
| BFP | Bichat’s fat pad | Buccal fat pad |
| SOOF | Sub-orbicularis oculi fat | None |

The intersection of these two lines determines the maximum point of projection of the convexity and this is called the zygomaxillary point. The convexity in the male and female differs significantly in extent and projection. In a female, the convexity extends to the upper lip but in the male the convexity is short and ends at the level of the projection of the nasal ala. In general, this outline gives to the male midface a more angular and bony look. Conversely, in the female, the large convexity gives an impression of softer and delicate features without significant angularity. It also shows a less bony facial appearance. One of the important goals of the midface rejuvenation is to create this reciprocal multi-curvilinear line of beauty or ogee line. The first step in the creation of this is to realize that you are working on a female or on a male midface.
Midface remodeling and lifting via an intraoral incision alone can be used in younger patients. This procedure, called endomidface, can be done via a single intraoral 2.5 cm incision. Inclusion of the temporal component of the forehead, however, provides superior results and this procedure is called endo-temporo-midface. This is used in most older patients because the added lift and remodeling of the lateral periorbita and the glabrous portion of the temple with the inclusion of the temporal dissection is needed. Crowding and folding of tissue in those areas otherwise can be an unsightly side-effect of the surgery.
Initial temporal dissection
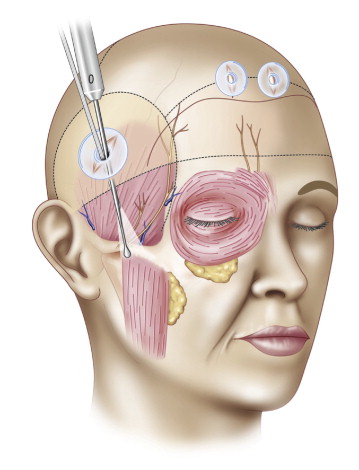
Surgery starts with a 2 cm long temporal incision made within the hair bearing portion of the temporal scalp ( Figure 12.5 ). This incision is normally located at a tangent of a line joining the nasal ala and lateral orbital rim extending into the temple. It is usually located 3 cm horizontally and 3 cm vertically inside the temple hairline. Caution is advised not to make the incision too anteriorly in hairy patients so that the incision is close to where the branches of the frontal nerve travel, or to make it too posteriorly or superiorly in patients with thin hair so that the temporal suspension can overshoot the area where the temporal fascia proper (TFP) also called the temporalis fascia is located. After the incision is deepened to identify the glistening fascia of the TFP, dissection proceeds under direct visualization for several centimeters radius ( Figure 12.6A ). The silastic port protector designed by Guyuron is introduced at the incision for protection of the hair follicles and to avoid penetration of hair into the surgical wound. Further dissection is done under endoscopic visualization. A 5 mm diameter, 30 degree down-angled endoscope is used over which the ‘Ramirez cobra sleeve’ is applied (Snowden Pencer Inc, Tucker GA).
Release of tissues
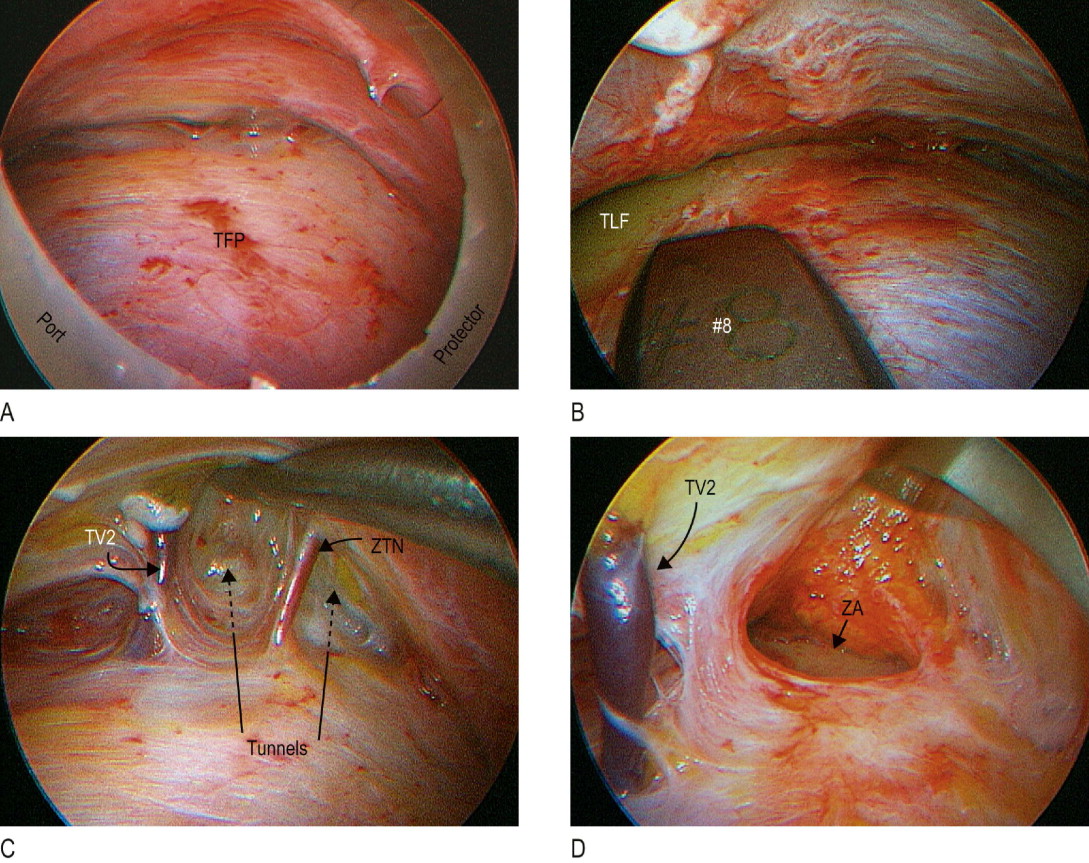
With a #4 Ramirez periosteal elevator, the soft tissue is elevated until the temporal line of fusion and the area of the sentinel vein also called the temporal vein #2 (TV2) are identified. Posterior to the axis where the temporal branch (frontal nerve) of the facial nerve is located, dissection can continue to the root of the helix and posterior zygomatic soft tissue area. Although the central forehead is not usually touched, elevation of the tail of the brow and crow’s feet area is most often needed; therefore dissection should continue for 1–2 cm medial to the temporal line of fusion (TLF) and the lateral one-third of the brow area. For this, a curved Ramirez periosteal elevator #8 is used ( Figure 12.6B ). This splits the periosteal and temporal fascia attachments to the TLF. Thus, dissection under the superficial temporal fascia (STF) and over the TFP in the temporal continues under the periosteum of the frontal bone.
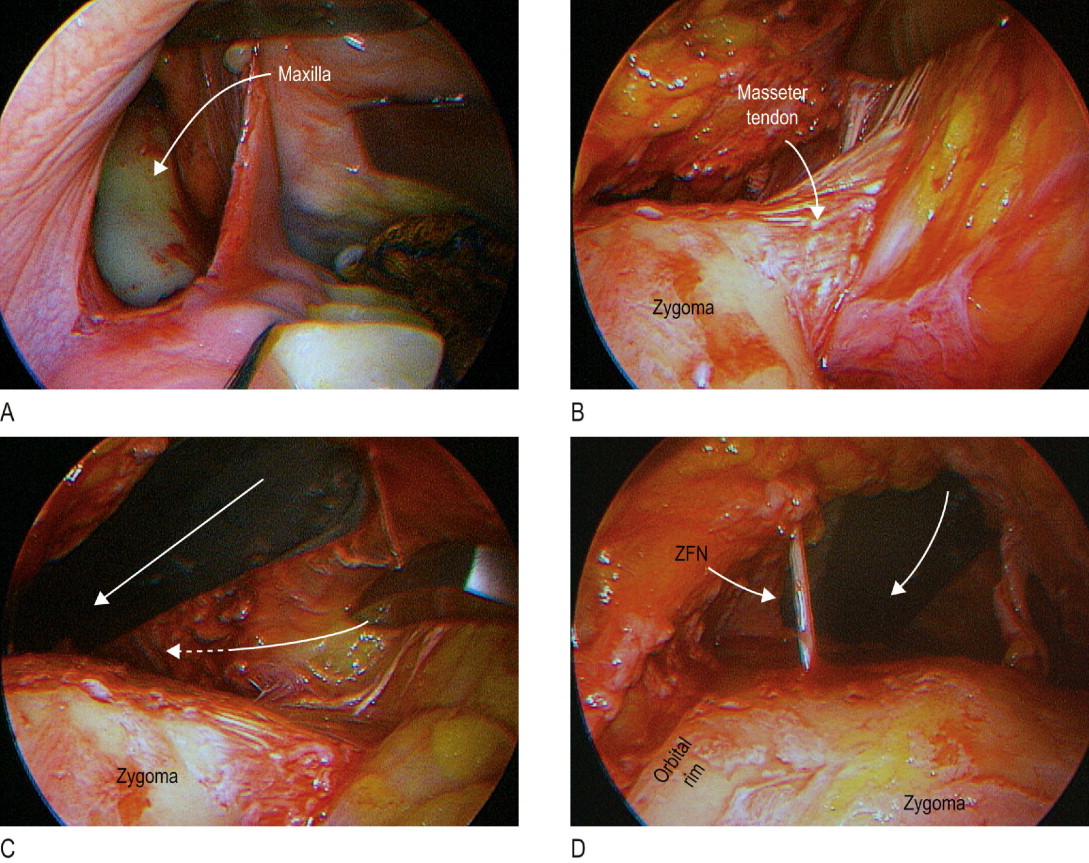
Inferiorly, dissection continues to incise the lateral extent of the arcus marginalis and to elevate the galea off the lateral orbital rim periosteum. In other words, laterally the periosteum of the orbital rim is left intact. The 0 Ramirez periosteal elevator is then introduced to dissect toward the zygomatic arch. Tunnels anterior to the TV2 and in between this and the zygomatic temporal nerve (ZTN) are made ( Figure 12.6C ). Near the zygomatic frontal suture line a small vein (TV1) is usually split and electrocoagulated. Through the mentioned tunnels and with the aid of the endoscope and the Ramirez periosteal elevator #9 the zygomatic arch periosteum is elevated entering just at the superior border of the arch and on its anterior one-third ( Figure 12.6D ). When this plane of dissection has been indentified, lateral dissection over the middle third of the zygomatic arch is performed.
Rarely, the lateral third of the arch is elevated. This lateral zygomatic arch dissection is needed when a more lateral vertical lift of the cheek is required. If the masseter tendon or muscle fascia is easily elevated from the temporal approach this can be continued 1–2 cm inferiorly. If not, this part of the dissection should proceed from the intraoral approach. The intraoral incision is obliquely or vertically oriented at the level of the first to second pre-molar away from the opening of the Stenson’s duct caruncle in the mouth ( Figure 12.7A ). The ends of the incision can be extended in a Z shape. Only the mucosa is initially incised with a #15 blade. The overlying buccinator muscle is bluntly separated when deepening of the incision toward the maxillary bone. With a #9 Ramirez periosteal elevator and using an Autfricht lighted retractor subperiosteal dissection is performed until the inferior orbital nerve is identified. Medially, dissection continues to the pyriformis aperture and laterally to the masseter tendon insertion into the malar bone.