Leg Ulcers
John T. Crissey
(ICD-9 707.1)
Symptoms and Signs
Venous Ulcers (Stasis Ulcers)
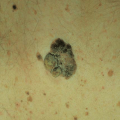
Venous ulcers are more common in women; patients are usually middle-aged or older, often with a history of thrombophlebitis. Although pain and tenderness associated with venous ulcers may be pronounced, symptoms are usually less prominent than one might expect from the clinical appearance. Venous ulcers often follow a minor injury. They are usually unilateral, involving the lower third of the leg and ankle, especially the malleoli. The borders are sharp and often irregular. The surrounding skin may be markedly thickened, hyperpigmented, and pebbly. Chronic lymphedema is also often present. The base of the ulcer, which bleeds easily when disturbed, is made up of granulation tissue and necrotic slough in varying proportions (Fig. 70-1).
Signs of chronic venous insufficiency in the areas surrounding the ulcers provide clues to the diagnosis: red–brown speckles of hemosiderosis against the more uniformly brownish background of hyperpigmentation, along with scattered purpuric macules. Eczematous changes—patchy areas of brighter erythema, moist papules, scaling, serous crusting, and excoriations—may also be present.
Arterial Ulcers (Ischemic Ulcers)
Atherosclerosis is the usual cause of arterial ulcer (AU) in the elderly. Men are more susceptible than women. AUs are uncommon before middle life. Pain is the outstanding feature, and intermittent claudication is often prominent. Arterial ulcers are usually sharply defined and round, as if punched out (Fig. 70-2). They tend to be smaller than venous ulcers and may be deep enough to expose muscle and tendons. The base is commonly covered with a necrotic slough. Pretibial areas, toes, and dorsa of the feet are the favored sites.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


