Lateral Tarsal Strip Canthoplasty
Richard H. Caesar
DEFINITION
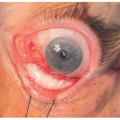
Any lower eyelid laxity or frank ectropion of the lower eyelid that results in a failure of the lower eyelid to sit smoothly against the globe can lead to symptoms of epiphora, discomfort, and poor appearance.
Lower eyelid tightening is a crucial component of the treatment of lower eyelid ectropion of any cause.
Any entropion of the lower eyelid (inversion of the lower eyelid) will usually have lower eyelid laxity as a component of the etiology. Lateral tarsal strip can be used to address this laxity with additional steps to reattach the lower eyelid retractors.
Lateral tarsal strip canthoplasty is a powerful technique for lower eyelid tightening.1
ANATOMY
The lateral canthal tendon attaches the lateral ends of the tarsi to Whitnall tubercle, 2 mm posterior to the lateral orbital rim formed by the zygomatic bone.
It is the origin of the palpebral and pretarsal orbicularis muscle fibers that pass to the medial canthal tendon.
PATHOGENESIS
Common causes of acquired ectropion include age-related laxity and cicatricial changes resulting from iatrogenic causes, trauma, or burns.
A paralytic ectropion results from a loss of innervation to the orbicularis muscle and facial elevators.
Mechanical ectropions are rare and result from external forces such as eyelid tumors.
NATURAL HISTORY
Acquired ectropion in most cases can only be corrected with surgery.
Notable exceptions are temporary paralytic ectropion that can have full spontaneous recovery and mild cicatricial ectropion secondary to dry skin or dermatitis. Intensive treatment with emollients, anti-inflammatory agents, and massage can, on occasion, fully resolve the ectropion.
Acquired entropion (lower eyelid inversion with abrading of the conjunctiva/cornea by the eyelashes) always requires surgery for a permanent solution.
PATIENT HISTORY AND PHYSICAL FINDINGS
Notable patient history and physical findings that should be assessed include appearance, epiphora, and pain/discomfort.
Lower eyelid laxity with marginal eversion and conjunctival exposure should be assessed.
Also assess secondary inflammation and thickening of the eyelid margin.
Exclude tethering or cicatricial changes of the skin, lower eyelid retractors, or conjunctiva. Exclude mechanical cause and paralytic cause.
IMAGING
Imaging is not usually required, but orbital MRI may be useful to identify the cause of unusual cicatricial changes to the lower eyelid retractors.
NONOPERATIVE MANAGEMENT
Surgery may be avoided with a resolving paralytic ectropion and a treatable mild cicatricial ectropion.
If the patient does not want surgery or is unable to have surgery, the eye can be kept comfortable by means of intensive ocular lubricants day and night. We recommend preservative-free hyaluronic acid-based lubricants during the day and white soft paraffin at night.
Involutional entropion can be treated with injection of botulinum toxin to the lower orbicularis.2
SURGICAL MANAGEMENT
Lower eyelid laxity and frank entropion and ectropion repair requires lower eyelid tightening. This can be achieved by many different techniques to include wedge resection, skin-sparing wedge resection, lateral canthopexy and lateral tarsal strip.
Concurrent lower eyelid blepharoplasty, skin grafting, heteropalpebral flap, medial retractor repair, central retractor repair, and surgery to the medial canthal tendon may also be required.
The lateral tarsal strip remains one of the most powerful techniques to tighten the lower eyelid.
Preoperative Planning
The surgeon should define the position of the incision, the degree of eyelid shortening required, and the angle of placement of the deep suture to the orbital rim.
Concurrent additional procedures should be determined.
The vast majority of patients are comfortable with local anesthesia alone, but sedation and general anesthesia should be available when required.
Positioning
The patient is most comfortable lying reasonably flat with a cushion under the head and knees.
The surgery can be done with the patient sitting if required.
The surgeon sits to the side of the patient.
TECHNIQUES
▪ Markings and Anesthesia
Mark the incision from the lateral canthal angle to extend 10 to 12 mm laterally and inferiorly following the most obvious rhytide (TECH FIG 1A).Related posts:
 Mandible Reconstruction With Fibula Flap With Templates
Mandible Reconstruction With Fibula Flap With Templates
 Lower Lip Reconstruction With the Nasolabial Flap
Lower Lip Reconstruction With the Nasolabial Flap
 Lower Eyelid Reconstruction With Palatal Grafts
Lower Eyelid Reconstruction With Palatal Grafts
 Reconstruction of the Ear Lobe
Reconstruction of the Ear Lobe
 Pectoralis Major Flap for Pharyngeal Reconstruction
Pectoralis Major Flap for Pharyngeal Reconstruction
 Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers
Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


