Introduction
The lateral arm flap (LAF) is a reliable septofasciocutaneous flap for local and free tissue transfer. Song et al. in 1982, Cormack and Lamberty in 1983, and Katsaros et al. in 1984 first reported the advantages of the conventional LAF. In its original design, the flap extends from the insertion of the deltoid muscle to the lateral epicondyle. Katsaros et al. and Kuek and Chuan were first to report the clinical use of an “extended” lateral arm flap (ELAF) in 1991. The ELAF is a LAF that includes an extension over and beyond the lateral epicondyle. The LAF/ELAF presents numerous advantages including a constant vascular anatomy, based on a terminal branch of the profunda brachii artery, minimal donor site morbidity, and a great variability in design. The LAF/ELAF can be employed for reconstruction in the lower and upper extremities and especially in the head and neck region.
Flap Anatomy (see Fig. 46.1 and Fig 12.4 , Fig 12.5 , Fig 12.22 , Fig 12.23 )
Arterial and Venous Supply of the Flap ( Fig. 46.1 and Fig 12.4 , Fig 12.5 )
Dominant:
radial collateral artery (RCA) of the profunda brachii artery (PBA)
Length: 6 cm (range 4–8 cm)
Diameter: 1.5 mm (range 1–3 mm)
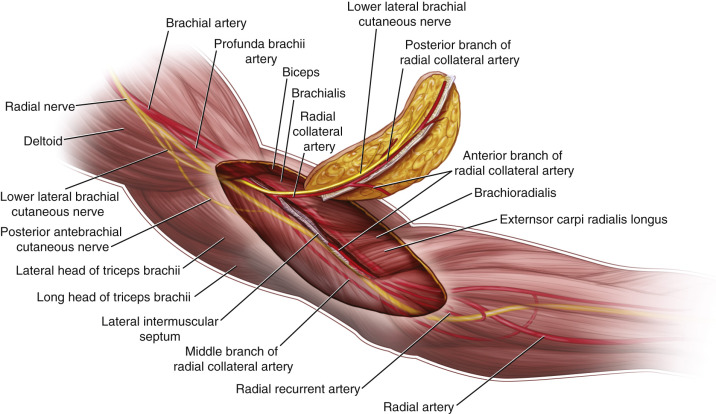
The main branch of the RCA that supplies the flap is the PRCA. This posterior branch arises from the RCA at the anterolateral border of the triceps muscle and runs distally through the lateral intermuscular septum between the triceps posteriorly and the brachialis and brachioradialis anteriorly. It supplies the overlying flap skin by four or five septocutaneous perforators along the intermuscular septum, and empties into the epicondylar and olecranon plexus. The most distal septocutaneous perforator typically branches off at approximately 4 cm proximal to that prominence.
The use of the ELAF, including the proximal forearm region, enables a lengthening of the pedicle up to 16 cm as compared with the conventional LAF (6 cm). It is important to include the distal septocutaneous perforator above the lateral epicondyle, harvesting the ELAF.
Minor:
anterior radial collateral artery (ARCA)
Length: 3 cm (range 2–6 cm)
Diameter: 0.8 mm (range 0.5–1.5 mm)
Minor:
interosseous recurrent artery (IRA) and recurrent radial artery (RRA) (important for distally pedicled flap)
Length: 3 cm (range 2–6 cm)
Diameter: 0.8 mm (range 0.5–1.5 mm)
Venous Drainage of the Flap
Primary:
venae comitantes of the radial collateral artery and its posterior branch
Length: 6 cm (range 4–8 cm)
Diameter: 2.5 mm (range 1.5–3 mm)
Venous drainage is supplied by two (75%) and less frequently by one (25%) venae comitantes.
Secondary:
cephalic vein
Length: 20 cm (range 15–25 cm)
Diameter: 6 mm (range 4–10 mm)
The cephalic vein itself or smaller braches can be included in the anterior part of the flap during dissection to provide augmented drainage.
Flap Innervation ( Fig 12.22 , Fig 12.23 )
Sensory:
the lower brachial cutaneous nerve (LBCN) is a primary sensory branch of the standard skin territory of the LAF
The posterior antebrachial cutaneous nerve (PACN) supplies a more distal skin territory, inferior to the lateral epicondyle, used for the ELAF.
Motor:
this is a septofasciocutaneous flap
Flap Components
The LAF/ELAF is generally harvested as a septofasciocutaneous flap, but it can also be elevated as a pure fascial flap. In addition, it can include a fragment of the posterolateral distal humerus as an osseofasciocutaneous flap. It is possible to integrate a segment of the lateral head of the triceps muscle and also a segment of vascularized triceps tendon. Enclosing the ARCA also enables integration of a segment of brachialis or brachioradialis muscle. The inclusion of the LBCN or PACN enables the design of a neurosensory flap.
Advantages
- •
The LAF/ELAF is a reliable fasciocutaneous flap for local and free tissue transfer with constant vascular anatomy.
- •
In the elevation of the LAF/ELAF, there is no risk to the vascular supply of the hand, because the LAF/ELAF contains a terminal branch of the PBA.
- •
Dissection is easy with the patient in supine as well as in prone position.
- •
There is only minimal donor site morbidity with generally direct closure up to a width of 8 cm in elderly patients.
- •
The unique vascular plexus in the elbow region allows great variability in design.
- •
Using the ELAF, there is increased skin availability and pliability of thin proximal forearm skin, but, above all, a long vascular pedicle can be obtained. Therefore, the ELAF is one of the best alternatives for the radial forearm flap.
- •
The variability in fasciocutaneous thickness (i.e., upper arm – thick; proximal forearm – thin) enables the use of this flap in two different regions according to defect requirements. In addition, the versatility of this flap is enlarged by the potential inclusion of vascularized osseous, nerve, or musculotendinous tissue.
Disadvantages
- •
Transection of the LBCN and PACN will result in a sensory deficit in the posterolateral side of the arm and forearm. This area of hyposensibility is significantly reduced after 6 months because of ingrowth of the surrounding cutaneous nerve.
- •
Donor site complications are described, including lateral epicondylar pain, hyperesthesia of the proximal lateral forearm skin caused by damage to the posterior cutaneous nerve of the forearm during raising of the flap, temporary radial nerve palsy, and a decreased range of motion.
- •
The radial nerve, coursing deep to the PBA in the region of the spiral groove, is endangered during proximal dissection of the vascular pedicle.
- •
Using the LAF/ELAF as a free flap, the small diameter of the flap’s vessels, especially the veins, is disadvantageous, particularly when the pedicle is ligated distally from the branching of the ARCA.
- •
The reverse flap requires retrograde flow, which can result in inadequate flap perfusion. A 180° flap rotation may additionally lead to venous insufficiency.
- •
Hair growth in the skin territory of the ELAF in some male patients may also be a problem, especially for head and neck reconstruction.
- •
The flap, especially the LAF, is thick in overweight individuals. However, the ELAF is always thin and pliable.
Preoperative Preparation
Preoperatively, the surgeon has to ensure that there has been no prior trauma or operative intervention at the donor region that could endanger the vascular supply of the LAF/ELAF. In cases of trauma, consideration should be given to performing a Doppler sonography or in very rare situations, an angiogram (CT angiogram) to determine the blood supply. Extended local scarring can necessitate the choice of another donor site. The hair at the operative field, especially at the male forearm region, has to be trimmed or removed by laser. There is no size or age limitation of the patients. In elderly patients, with relaxed arm skin, the donor site can even be closed directly up to 8 cm. While the upper arm and forearm territory provide one of the thinnest flaps available, in obese individuals it can still be bulky. However, a thin fascia flap covered with split-thickness skin graft can be raised in even the most obese individuals. If operability is ensured and there is no evidence for vasculopathy, preventing microsurgical intervention, no contraindication for the surgery exists.
Flap Design
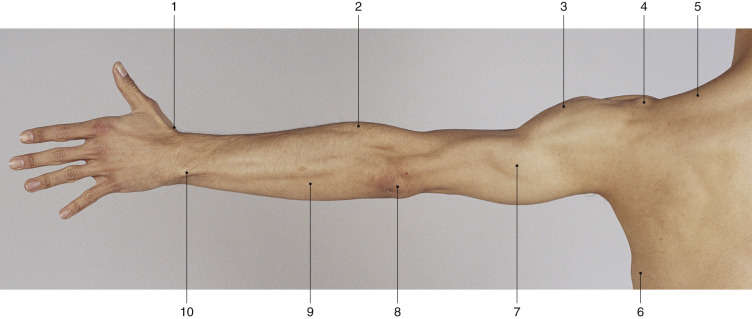
Anatomic Landmarks ( Fig. 46.2 )
The bifurcation of the PBA is visualized at the level of the deltoid insertion beneath the lateral caput of the triceps muscle. Marginally distal, the RCA, as the pedicle’s basis, divides into PRCA and ARCA before appearing at the anterolateral aspect of the triceps. The pedicle’s axis passes along the lateral intermuscular septum, which is located between the brachialis and brachioradialis muscle on the anterior side and the lateral head of the triceps muscle on the posterior side. The skin island of the conventional LAF is located between the insertion of the deltoid muscle and the lateral epicondyle. The axis of the skin island of the ELAF at the forearm is centered on a line between the lateral epicondyle and the processus styloideus radii.
General Thoughts about Flap Design
The flap design depends on the defect that has to be covered. According to the size of the defect, the dimensions of the LAF can be extended over and beyond the lateral epicondyle (ELAF). The distal extension of the ELAF can reach up to 15 cm beyond the epicondyle. The combination of LAF and ELAF can result in flap dimensions of about 35 cm length. Finally, the possible length of the flap depends on the patient’s age, body size, and local tissue situation. The surgeon can use the thicker fasciocutaneous tissue of the upper arm, the thinner extended part of the ELAF, or both, according to the defect requirements. Generally, it is sufficient to raise only the extended part of the ELAF, particularly as the ELAF provides a thinner and more pliable skin paddle than the LAF. In addition, the extension of the LAF provides a longer pedicle of the flap.
Width generally should not exceed 6 cm to allow for primary closure of the donor defect. In combination with Z-plasties, donor defects up to 8 cm can be closed directly.
Special Considerations
Head and Neck Reconstruction
In 3-dimensional defects with loss of bone, muscle, or nerve tissue, the LAF/ELAF enables the inclusion of vascularized bone, muscle, or nerve tissue (see below). Compared with the radial forearm flap, the ELAF, with its very long pedicle and its thin, pliable skin, is perfectly indicated for intraoral reconstruction. Sometimes laser hair removal has to be performed before this ELAF application.
Extremity Reconstruction
- •
Soft tissue defect with a bone defect: a vascularized segment of the distal humerus may be included.
- •
Soft tissue defect with a 3-dimensional defect: a vascularized segment of the lateral head of the triceps, brachialis, or brachioradialis muscle may be included.
- •
Soft tissue defect with a peripheral nerve defect: the PACN can be harvested with the flap as a vascularized nerve graft.
- •
Soft tissue defect with substantial loss of a tendon: for tendon grafting, a vascularized part of the triceps tendon may be integrated with the segmental muscle flap.
Difference in Design, If Any, When Performing the Flap as Pedicled or Free
Generally there is no difference in design when performing the flap as pedicled or free. Only the design of the reverse LAF differs, because of its other pedicle, as described below.
Flap Dimensions
Skin Island Dimensions
Lateral Arm Flap
Length: average 12 cm (range 5–20 cm),
Width: average 6 cm (range 3–12 cm), maximum to close primarily: 8 cm
Thickness: average 10 mm (range 5–35 mm)
Widths up to 8 cm can be closed primarily in elderly patients. The thickness of the flap varies with the donor site (proximal thick fat layer vs distal thin fat layer).
Extended Lateral Arm Flap
Length: Average 12 cm (range 5–35 cm),
Width: Average 5 cm (range 2–10 cm),
Thickness: Average 5 mm (range 5–15 mm)
The use of the ELAF as an extension of the LAF to the antebrachial region allows the elongation of the skin island and the harvest of thinner skin tissue in comparison to the brachial area. According to the defect requirements, the surgeon can also use the thinner and more pliable skin paddle of the ELAF alone.
Muscle Dimensions
Triceps Muscle
Length: Average 10 cm
Width: Average 2.5 cm
Thickness: Average 1 cm
Brachialis Muscle
Length: Average 4 cm
Width: Average 2 cm
Thickness: Average 2 cm
Brachioradialis Muscle
Length: Average 6 cm
Width: Average 2 cm
Thickness: Average 2 cm
This flap is mainly a fasciocutaneous flap but part of the triceps muscle and small parts of the brachialis or brachioradialis muscle could be included, as filling material for deep defects. The dimension of the harvested muscle tissue especially depends on the patient’s constitution. Using the larger part of these muscles will produce significant donor site morbidity.
Bone Dimensions
Humerus
Length: Average 6 cm (range 2–15 cm)
Width: Average 1 cm (range 0.5–1.5 cm)
Thickness: Average 1 cm (range 0.5–1.5 cm)
The inclusion of a bone fragment necessitates immobilization for 2–3 weeks to avoid fracture of the distal humerus.
Tendon Dimensions
Triceps Tendon
Length: Average 6 cm (range 3–10 cm)
Width: Average 1 cm (range 0.5–2.5 cm)
Nerve Dimensions
Lower Brachial Cutaneous Nerve/Posterior Antebrachial Cutaneous Nerve
Length: Average 14 cm (range 12–16 cm)
The flap can include a vascularized nerve graft in combination with soft tissue reconstruction. The nerve graft on its own does not have a pedicle; therefore, it has to be harvested as a composite flap with the main pedicle of the LAF/ELAF.
Flap Markings ( Fig. 46.3 )
The skin island’s axis of the conventional LAF is centered over a line between the mid-deltoid to the lateral epicondyle. The insertions of the deltoid muscle and the lateral epicondyle mark the proximal and distal edge. The proximal edge of the conventional LAF flap could be prolonged over the deltoid muscle. However, this area is difficult to close primarily and hypertrophic scar formation is usual.
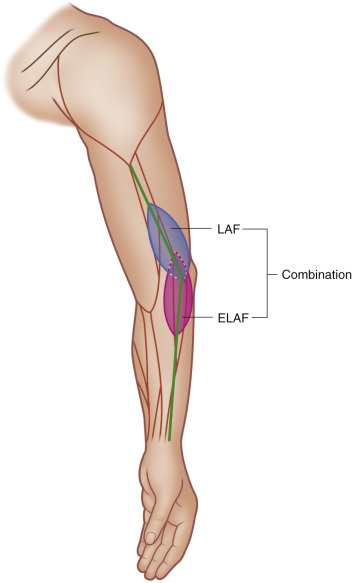
The ELAF is an LAF that includes an extension of the flap’s skin area over and beyond the lateral epicondyle. In our experience, the maximal distal extension can reach 12–15 cm beyond the lateral epicondyle at the radial proximal forearm region without problems with blood supply. If only the forearm skin of the ELAF is used, the skin island ends proximal at the level of the lateral epicondyle. The skin island positioned over the lateral epicondyle is also a common design. The width is planned in accordance with the requirements of the defect’s dimensions.
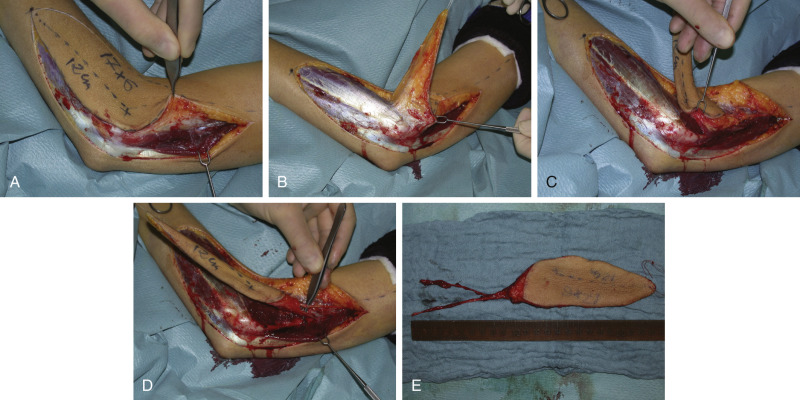
Technique of Flap Harvest
Lateral Arm Flap
After the flap is outlined, the dissection is begun in a bloodless field (use the sterile tourniquet applied very proximal and posteriorly to achieve better access to the vascular pedicle) postero-proximally ( Fig. 46.4 ). The incision will be performed posterior to the lateral intermuscular septum over the lateral head of the triceps muscle. After exposure and incision of the deep fascia, the flap is elevated on the muscular level until the intermuscular septum with the septocutaneous perforators becomes visible, exposing the lateral head of the triceps muscle. The overlying fascia is fixed with two stitches to the skin to avoid a separation of skin and fat layer. After that, dissection proceeds anteriorly until the intermuscular septum is reached, exposing the brachialis and brachioradialis muscles. The septocutaneous perforators are visualized superficial to the deep fascia. Afterward, the distal fascia is incised to the level of humeral periosteum and the intermuscular septum is now separated, with periosteum, from the humerus proximally to the level of deltoid insertion.