Labbé Procedure: Lengthening Temporalis Myoplasty
Daniel Labbé
Pierre Guerreschi
DEFINITION
Facial paralysis sequelae might lead to major physical and social consequences that can drive patients to isolation, unemployment, and depression.
The facial asymmetry observed at rest is aggravated by facial motion.
ANATOMY
All facial muscles can be affected.
Muscles on the paralyzed side do not contract effectively and can even be the object of erratic cocontractures.
After a few years, they can even spasm in an intermittent or permanent manner, leading to facial twitch or hemifacial spasm.
Muscles on the opposite side tend to be overactive and thus aggravate the facial asymmetry.
PATIENT HISTORY AND PHYSICAL FINDINGS
We differentiate three different clinical pictures: complete facial paralysis, facial paresis, and spams with secondary muscle overactivity. These different clinical pictures can occur simultaneously successively over time.
Complete facial paralysis leads to both static and dynamic asymmetries.
At rest, the median line is offset to the healthy side. The forehead is relaxed, smooth, and inexpressive.
The eyebrow is droopy especially toward the outside; we often note a ptosis of the eyebrow’s outer corner aggravating an eventual dermatochalasis.
The lower eyelid is also impacted by the absence of muscle tone. It droops, leading to an eversion of the eyelid with an ectropion that varies according to the patient’s age.
The cheek is flaccid and distended.
The commissure droops.
Spontaneous facial animation unveils and aggravates the facial asymmetry.
Facial paresis mimics this clinical picture. When static, the facial symmetry might be almost normal, yet facial animation will unveil the asymmetry.
During the course of the pathology, some muscles can spasm, sometimes progressing to real contractures leading to hemifacial spasm.
This spasm can remain clonic and discreet or worsen and become a contracture, with varying degree of pain severity. It is associated with progressive motor impairment. It becomes more severe when the patient becomes emotional or stressed.
Several muscle groups can therefore be affected by spasms: the depressor labii inferior (DLI) muscles can be spastic, with at the forefront the depressor anguli oris (DAO)/platysma complex. The spasm of this muscle group prevents the elevation of the labial commissure.
On the healthy side, muscles often progress to overactivity.
The frontalis muscles mark forehead wrinkles and elevates the eyebrow on the healthy side, even at rest.
The levator anguli oris muscles are also frequently affected by offsetting the mouth toward the healthy side in an exaggerated manner.
The overactive DLI impairs elocution by everting the median labial line toward the healthy side.
Finally, the platysma neck cords are a sign of platysma muscle overactivity.
IMAGING
Imaging studies are rarely needed in patients with chronic facial paralysis or facial paresis.
In rare instances, brain MRI or CT scans may be necessary to rule out an intracranial cause of facial paralysis.
NONOPERATIVE MANAGEMENT
Botulinum toxin is largely used for all stages of facial paralysis and concerns all facial muscles.
It is particularly relevant because its action is very selective on the different muscle groups, yet its effectiveness is temporary.1 It allows for a fine action on the overactive muscles, especially the zygomaticus major and minor and the DLI, where myectomy procedures are more complicated to perform.2
In facial paresis, botulinum toxin can treat spasms and cocontractures.
Interestingly, when regularly treated, muscles become atrophied, and the therapeutic action of the botulinum toxin seems to last longer over time.
SURGICAL MANAGEMENT
Myoplasty techniques use the adjacent muscles with different innervations (V) to reanimate the functions normally provided by the paralyzed facial muscles.3 The first myoplasty was performed by Lexer with the masseter muscle at the beginning of the 20th century.
Some anatomic-pathologic data reinforce the choice of myoplasty surgery: simultaneous action with the muscles responsible for facial mimics, proximity, and presence of a trigeminofacial reflex.
The muscle mobilized during myoplasty must retain its own innervation and vascularization. It is essential to harvest enough quantity of muscle taking into account the location of its vascular and nerve pedicles.
Lengthening temporalis myoplasty first published in 19974 was inspired by the use of the temporalis muscle previously described.
This technique is a synthesis and an achievement, even if its author considers that the technique could still be improved (June 10, 2013). It consists of mobilizing the entire temporalis muscle freed from its distal and proximal insertions. Lowering the temporalis muscle through the buccal fat pad is associated with a lengthening of the muscle to the detriment of its posterior fibers.5
The insertion of the muscle transfer onto the lip is done according to the type of smile. Studying the patient’s smile during the preoperative period is essential to match as closely as possible the smile symmetry at rest and when contracting.
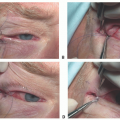
Preoperative Planning
The refined preoperative study of the patient’s smile on the healthy side helps determine the respective insertions of the zygomatic muscles and superficial and deep elevator muscles of the upper lip and also help refine the type of smile that needs to be achieved.
These anatomic landmarks identified on the healthy side will be transposed onto the paralyzed side as a mirror image to locate precisely the anchor points of the muscle flap.
The nasolabial fold and its exact shape, concave or straight, are also refined. The impaired nasolabial fold on the paralyzed side is restored by passively lifting up the lower lip and moving it backward.
This is performed when the patient is sitting down and then controlled again with the patient lying down.
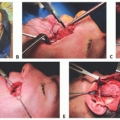
Positioning
The patient is positioned in the supine position, and orotracheal intubation is performed.
The tube is fixed to the lower incisors via a wire thread.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree