Introduction
In 1904, Wiilstein, in Germany, reported the first case of a jejunal flap. He used the jejunum as a pedicled flap to reconstruct the thoracic esophagus. In 1907, Roux, in France, described a successful staged reconstruction of the esophagus using the jejunum. The most common complication was necrosis of the most cephalad portion of the flap. As a result, pedicled jejunal flaps were generally restricted to esophageal defects below the inferior pulmonary vein.
In 1959, the jejunal free flap was the first reported successful free tissue transfer in humans. Seidenberg, without using the microscope, transplanted a loop of jejunum to the neck in a patient who had undergone a pharyngoesophagectomy. The jejunum has many anatomic advantages: it is tubed and lubricated, and has peristaltic activity; it also has a reliable blood supply. It is used for reconstruction of various defects, including the esophagus and vagina.
Regional Anatomy
Small Intestine
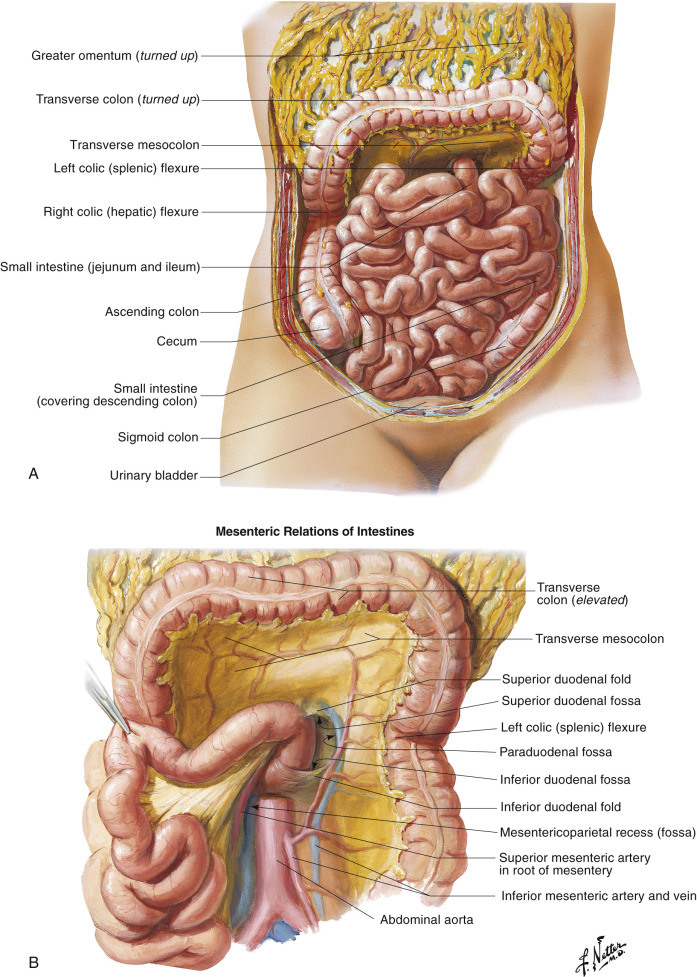
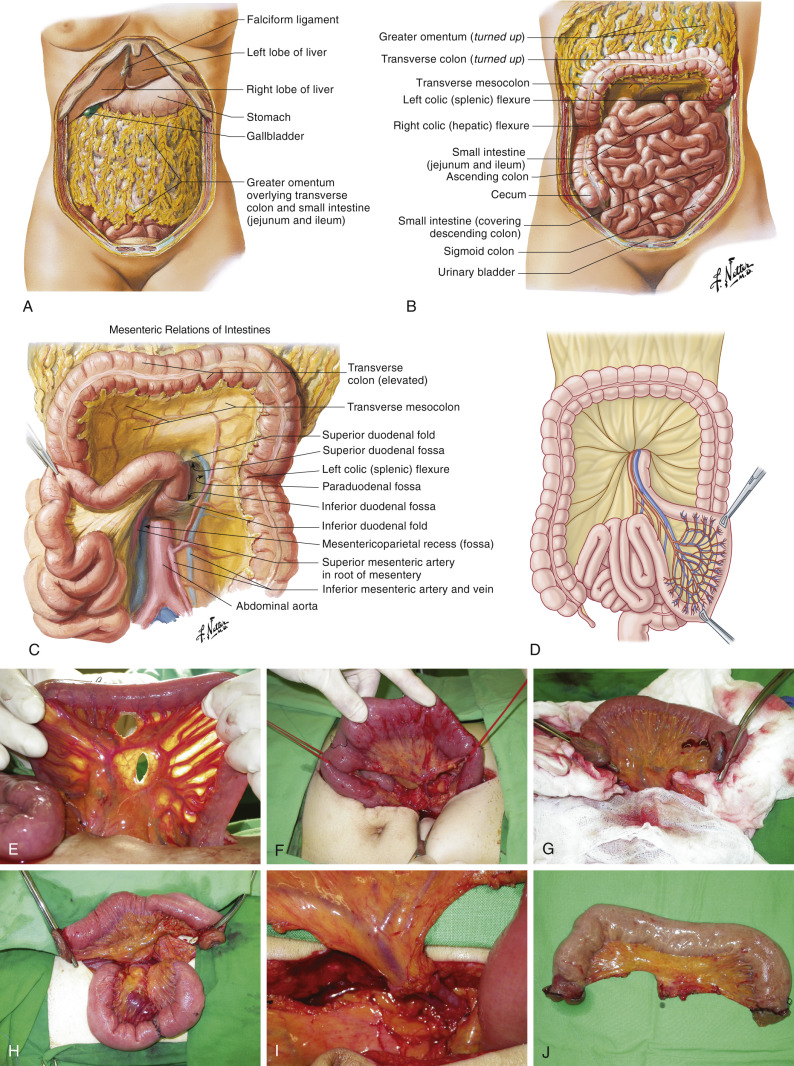
The small intestine extends from the pylorus to the ileocecal valve. It is composed of 3–7 m of duodenum, jejunum, and ileum ( Fig. 38.1 ). After the first 25 cm of duodenum, the remaining intestine is divided between jejunum and ileum; the proximal two-fifths is jejunum and the distal three-fifths is the ileum. Because the duodenum is a retroperitoneal structure and the jejunum is intraperitoneal, the beginning of the jejunum is easily recognized at the ligament of Treitz. The jejunum and ileum are attached to the posterior abdominal wall by the mesentery and are arranged in a series of loops.
Mesentery
The mesentery is fan-shaped and consists of two layers of peritoneum containing jejunum and ileum, blood vessels, nerves, lymph nodes, and fat ( Figs 38.1 , 38.2 ). The mesentery is attached superiorly to the posterior abdominal wall along an oblique line running from the left side of the body of the second lumbar vertebra to the right sacroiliac joint. This line of attachment is called the “mesenteric root.” The average length of the mesentery is 20 cm, being longer in the middle than at the proximal and distal ends.
Jejunum
The jejunum measures approximately 4 cm in external diameter and 2.5 cm in internal diameter. The jejunal intestinal wall is an important anatomic unit, distinguishing it from proximal stomach and duodenum and distal ileum. The jejunal wall contains thick circular folds extending into the lumen, perpendicular to the long axis. Unlike the stomach rugae, which disappear on distention, these circular folds are fixed. They decrease in number and size, progressing distally toward the ileum, and function to retard the passage of the food and to increase the surface area for absorption. Proximally, the circular folds are thicker and more numerous, the muscle layer is thicker, and the vascularity of the jejunal wall is greater. In the distal ileum, circular folds are absent and the circular muscle layer is thinner. In addition, the ileum diameter is smaller (external diameter 3.5 cm; internal diameter 2 cm) and the wall thickness is considerably less ( Fig. 38.3 ).
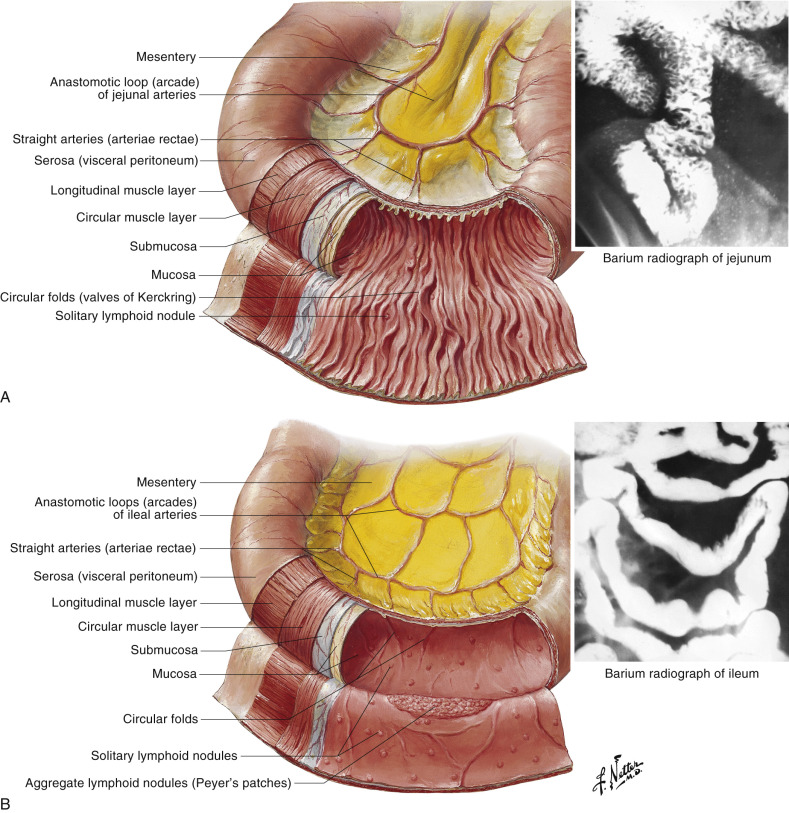
The intestinal walls are composed of:
- •
The serous layer formed of visceral peritoneum and subserous connective tissue
- •
The muscularis externa, consisting of a thin outer longitudinal layer and a thick inner circular layer
- •
The submucous layer consisting of nerves, blood vessels, and lymphatics in loose connective tissue
- •
Mucous membrane, which lines the jejunum and is also present in circular folds containing the intestinal villae, which are more concentrated and longer in the proximal jejunum.
The physiologic functions of the jejunum are chyme transport, digestion, absorption of nutrients, and production of gut-derived enzymes and hormones. Motility of the jejunum comprises two basic types of automatic movement: circumferential segmental contraction and peristalsis. After transplantation, however, the jejunal segment has a more varied motility, resulting in anterograde, retrograde, and peristaltic propulsion.
The clinical, reconstructive significance of jejunal anatomy lies in the intrinsic suitability of the jejunum for flap formation, because it has its own series of independent vascular territories.
Arterial Anatomy of the Region
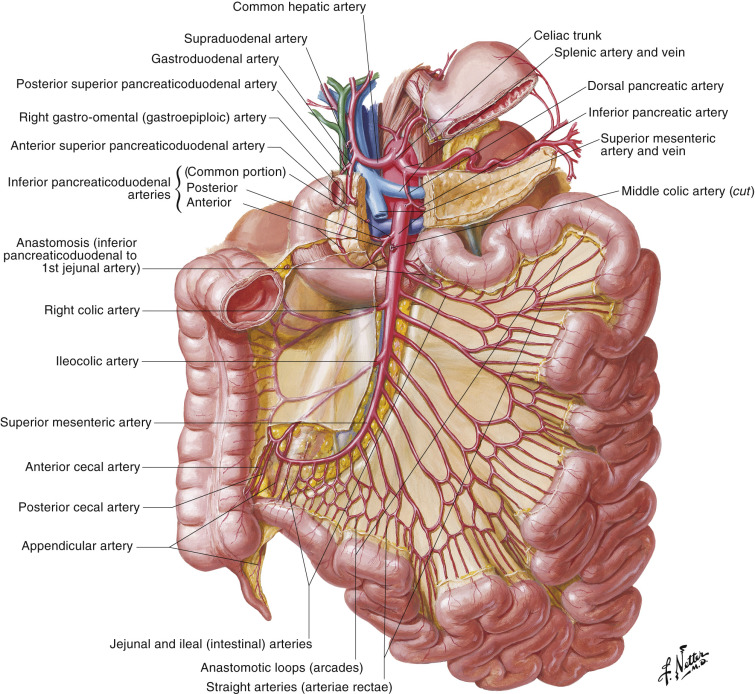
All blood supply of the small intestine and large intestine comes from the superior mesenteric artery and inferior mesenteric artery, both of which are direct branches of the abdominal aorta below the celiac artery. All arteries and veins run within the mesentery, along with lymphatic vessels and nerves ( Fig. 38.2 ).
Blood Supply of the Jejunum
The superior mesenteric artery arises from the anterior surface of the abdominal aorta, approximately 1 cm inferior to the celiac trunk, and supplies the entire small bowel and half of the large bowel ( Fig. 38.2 ). It courses in the mesentery toward the iliac fossa, where it forms an anastomosis with the ileocolic artery, one of its own branches. From the right side of the superior mesenteric artery arise, in descending order, the middle colic, right colic, and ileocolic arteries. The jejunal and ileal arteries arise from the left side of the superior mesenteric artery. Generally, the jejunal arteries are longer and fewer in number than the ileal arteries (see below).
Venous Anatomy of the Region
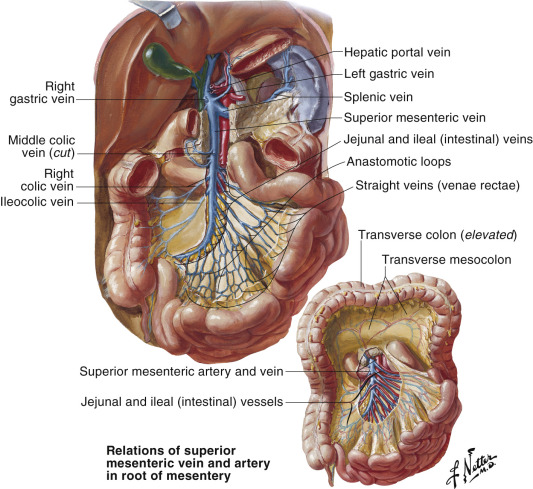
The veins that supply the jejunum and ileum accompany arterial branches of the same name and drain into the superior mesenteric vein. There are often two venae comitantes for each mesenteric artery. The walls of the veins within the mesentery route are thin and fragile ( Fig. 38.4 ).
Nerves in the Region
The nerve supply of the jejunum is both extrinsic and intrinsic. The extrinsic supply is autonomic, from the preganglionic parasympathetic, and postganglionic sympathetic branches of the celiac plexus. These nerves enter the jejunum through the mesentery along branches of the large vessels. The intrinsic nervous system is formed by the myenteric plexus of Auerbach, between the muscle layers and the submucosal plexus of Meissner. Fibers from the Auerbach plexus supply the muscularis externa, whereas Meissner’s plexus supplies the muscularis mucosa. Reflex arcs, involving afferent stimuli from the mucosal surface, and efferent motor activity within the myenteric plexus, seem to be responsible for the autonomous movements of the jejunum, when isolated from its extrinsic nerve supply. Such movements, however, are not significantly reduced by a complete myotomy.
Flap Anatomy
Arterial Supply of the Flap
The jejunum has its own series of independent vascular territories, corresponding to loops. These loops or segments, measuring up to 25 cm in length, are usually supplied by a single arteriovenous pedicle and maintain at least some autonomous cephalocaudad motility ( Fig. 38.2 ).
Jejunal Artery
Length: 5 cm (range 4–6 cm)
Diameter: 2.0 mm (range 1.5–2.5 mm)
The overall length of the pedicle varies between 15 and 20 cm, considering the course of the vessels within the mesentery. The overall length of the pedicle may be deceiving because there is an obligate relationship between the position of the main mesenteric vessels and the arcade and thus between the arcade and the segment of jejunum.
The blood supply network to the jejunum is a highly organized branching network composed of multiple, consecutive, tiered vascular loops called arcades. The primary-order arcades run parallel to one other within the layers of the mesentery ( Figs 38.2 , 38.5 ). These parallel vessels divide in two branches, one ascending and one descending, which course parallel to the intestine. These branches then unite with the adjacent branches coming from the closest jejunal arteries, thus forming an anastomotic arcade. The second-tier arcade is then formed off the primary arcade loop. In the same way, smaller vessels arising from the secondary arcades can form arcades of third or fourth order.
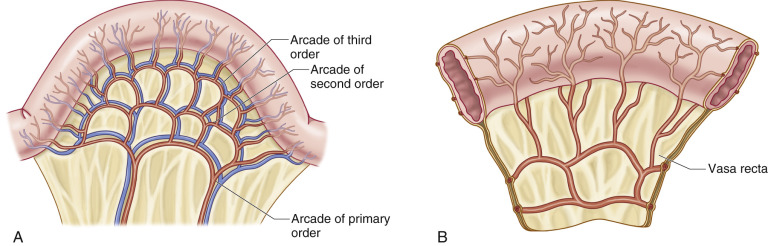
From the last arcade (which is the last arch parallel to the intestine) arise the vasa recta, which form the direct and final blood supply to the jejunum. The vasa recta are terminal vessels measuring approximately 4–6 cm ( Figs 38.2 , 38.5 ). One to two vasa recta supply a distinct area of jejunum (approx. 1 cm per vasa recta unit), thus the blood supply to the jejunum is described as segmental. These small vessels encircle the bowel and then circumferentially traverse only half of the intestine wall, between the muscle and the mucosa, forming a dense submucosal plexus. The least, although adequately, vascularized part of the bowel wall is along the antimesenteric border, 180° from the mesenteric attachment.
Depending on the length of the jejunum flap to be transferred, the vascular arches to be harvested must be carefully dissected toward the main jejunal branch off the superior mesenteric artery.
Venous Drainage of the Flap ( Fig. 38.4 )
Primary:
jejunal veins accompany arterial branches of the same name
Length: 5 cm (range 4–6 cm)
Diameter: 2 mm (range 3–4 mm)
The veins within the mesentery are thin and fragile and the utmost care has to be taken during dissection, especially when the mesentery has an abundance of fat ( Fig. 38.4 ).
Flap Innervation
Sensory:
There is no true sensory innervation of this flap. Bowel wall distention causes pain because of the overlying visceral peritoneum which has proprioceptor pain fibers. This reflex arc does not appear to be intact after transplantation.
Motor:
Afferent stimuli from the mucosal surface elicit efferent motor activity within the myenteric plexus, which is responsible for the autonomic peristalsis. The transplanted jejunum shows episodes of peristalsis and quiescence. The peristaltic wave follows the luminal distention of the jejunal segment. This peristalsis is not coordinated to distal esophageal motility when transferred to the esophagus.
Flap Components
The jejunum is harvested with its mesentery, which contains the vessels that supply it and the lymph nodes that drain it.
Advantages
- •
The tubed nature of the jejunum and its peristaltic activity provide functional benefits when used for pharyngeal and esophageal reconstruction, and minimize complications because of the low number of suture lines.
- •
Flap harvest is quick and simple.
- •
Jejunum diameter approximates that of the esophagus.
- •
As a free flap, the vascular pedicle can be lengthy (up to 15–20 cm), with vessels of suitable external diameter (artery 1.5–2.5 mm; vein 2–4 mm).
- •
The jejunum can be considered relatively sterile and is relatively free of intrinsic disease.
- •
The jejunum maintains its mucosa at long-term follow-up. There is no metaplasia/dysplasia that can be seen in the residual esophagus such as after the gastric pull-up procedure.
- •
The accompanying mesentery can be employed to cover vital neck structures and can provide a suitable bed for skin grafting if needed.
- •
The length of jejunum available for transplantation ranging 7–25 cm, based on only one pedicle.
- •
As a pedicled flap, the jejunum can replace the whole esophagus; however, in adult patients, it is necessary to supercharge the flap.
- •
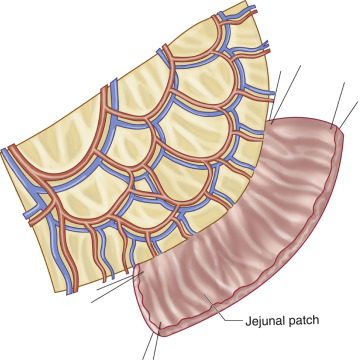
A portion of the jejunal segment may be split along its antimesenteric border, creating a vascularized patch, which is suitable for reconstruction of partial circumferential defects or for providing oral lining.
- •
When used as a buried flap, monitoring can be undertaken by exteriorizing a segment.
- •
The pedicled jejunum flap is ideal for vaginal reconstruction because it is mucosalized and tubular.
Disadvantages
- •
In experimental models, the jejunal flap may be more susceptible to harmful effects of ischemia. Clinically, an ischemia time of around 2 h has not shown adverse effects.
- •
The length of the pedicle may be deceiving because there is an obligate relationship between the position of the main mesenteric vessels and the arcade and thus between the arcade and the segment of jejunum.
- •
There is a mortality rate between 2.4% and 5% when using jejunal flaps for reconstruction of esophageal defects. This rate is similar to using gastric pull-up and colonic interposition.
- •
Fistula rates continue to range between 1.8% and 30%.
- •
The patient will require either a laparotomy or laparoscopy-assisted approaches to the abdomen, which carry their own inherent risks.
Preoperative Preparation
A thorough history and physical examination are performed, including previous intra-abdominal surgeries, medications that may interfere with coagulation, nutrition, and pulmonary status. No special preoperative studies are necessary. If intra-abdominal aortic vascular occlusive disease is suspected, an angiogram may be obtained, although this is rarely, if ever, necessary. Standard bowel preparation and bowel perioperative antibiotics are given. In general, obese patients have a fattier mesentery, which makes vessel dissection more precarious.
Contraindications to surgery are the presence of ascites, chronic intestinal diseases such as Crohn’s disease, and previous extensive jejunum harvestings. Harvest of jejunal flaps can be done more than once.
Flap Design
Anatomic Landmarks
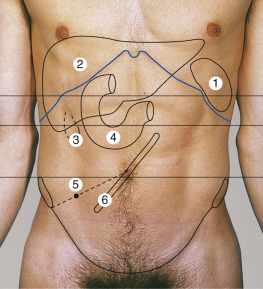
Standard midline laparotomy or laparoscopy-assisted incisions are used ( Fig. 38.6 ). Intra-abdominally, the ligament of Treitz in the left upper quadrant of the abdominal cavity marks the beginning of the jejunum. The superior mesenteric artery arises from the anterior surface of the abdominal aorta, approximately 1 cm inferior to the celiac trunk, and the jejunal and ileal arteries arise from the left side of the superior mesenteric artery.
General Thoughts About Flap Design
Depending on the location of esophageal resection, the patient can be evaluated for a free or a pedicled flap. As a free flap, the jejunum is generally used for microsurgical tissue transplantation to replace any part of the esophagus or hypopharynx. As a pedicled flap, it can be used to reconstruct the more distal, thoracic esophagus (interposition-like graft) or the vagina. The free jejunal flap is harvested from the second or third loop, whereas the fourth loop is usually used for a pedicled flap. This is because more length of pedicle can be obtained from the more distal jejunum by unfurling the bowel loops and elongating the arcades. For supercharging the pedicled flap, the third or second jejunal artery is used. If only a patch is required, the antimesenteric border of the jejunum can be opened and used reliably as a patch esophagoplasty.
Special Considerations
Jejunum as a Conduit ( Case 38.2 )
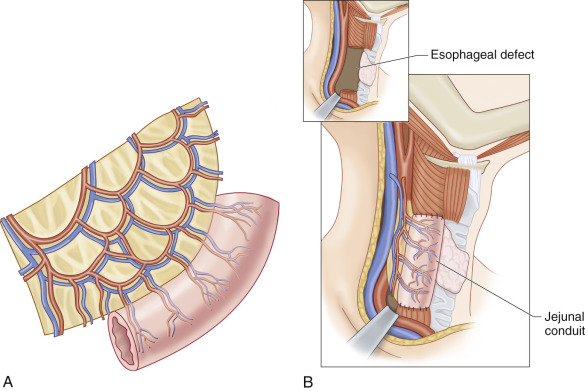
The jejunum is generally used as a conduit for circumferential reconstruction of esophageal, hypopharyngeal, and vaginal defects ( Fig. 38.7 ). There is no size mismatch between the cervical esophagus and jejunum, so no special design of the segment is required.
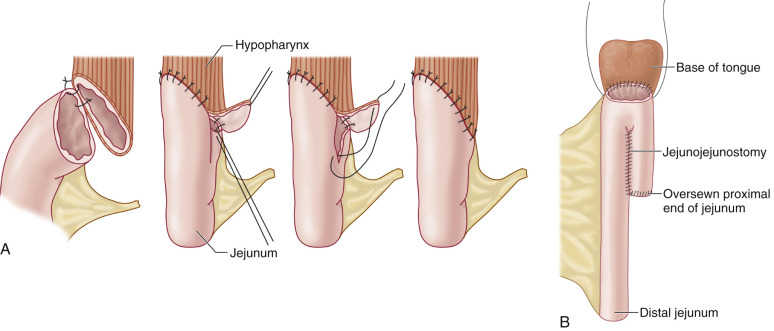
However, for oropharyngeal resection, the jejunum must be tailored to match the much larger oropharynx ( Fig. 38.8 ). The options are:
- •
Adapt the diameter of the hypopharynx.
- •
Adapt the shape of the jejunum through several maneuvers such as fish-mouth-type opening: the antimesenteric border of the jejunum is opened enough to create a better size match. The problem with this technique is the possibility of kinking.
- •
Double-barreled jejunum: the jejunum is folded and a side-to-side jejunostomy using a gastric stapling device is performed on the antimesenteric border. This is performed on the proximal aspect of the flap.
After radical surgery for cancer, a pedicled segment of jejunum can be utilized as a pouch to reconstruct the vagina: the upper end of the conduit is closed and the lower end is sutured at the perineum to the remnant of vagina.
Jejunum as a Patch
The jejunum can be used as a patch if there is a partial defect of the hypopharynx, a mucosal defect of the oral cavity, after esophagoplasty or after release of a focal stricture. When the jejunum is used for non-circumferential reconstruction, similar to a patch flap, it is split along the antimesenteric border. This patch can be transferred as either a pedicled or free flap ( Fig. 38.9 ).
Difference in Design, if Any, When Performing the Flap as Pedicled or Free
As a free flap, the second or third loop is usually harvested, based on the second or third jejunal artery. For a pedicled jejunum, the fourth jejunal loop is harvested and the fourth jejunal artery functions as the distal vascular pedicle to the mobilized jejunal conduit. The third jejunal artery is ligated and divided close to its origin from the superior mesenteric artery for supercharging. The mesentery of the jejunum is then divided at the serosal border between the second and third jejunal arteries, allowing the conduit to completely unfurl. This straightens the sinusoid turns in the small bowel caused by a naturally foreshortened mesentery.
Flap Dimensions
Any length of jejunum 7–25 cm may be transferred on one vascular pedicle. The bowel lumen diameter is 3–5 cm.
Flap Markings
Abdominal incisions are marked ( Figs 38.6 and 38.10 ). After identification of the jejunum segment, the proximal and distal ends must be marked so that the segment is transferred in the same isoperistaltic anatomic orientation.
Patient Positioning
The patient is placed in the supine position. In cases of esophageal reconstruction, two teams work simultaneously: one team prepares the neck recipient site, while the abdominal team harvests the jejunum.
Anesthetic Considerations
The patient is given general endotracheal anesthesia.
Technique of Flap Harvest
Harvesting Jejunum as a Free Flap ( Fig. 38.10 )
Either a midline laparotomy or laparoscopy-assisted incisions are made ( Fig. 38.10A ). After reflecting the transverse colon and stomach superiorly, the ligament of Treitz is identified in the left upper quadrant ( Fig. 38.10B,C ). The small bowel is followed to approximately 40–60 cm below the ligament of Treitz ( Fig. 38.10D ), where the vascular arcades are evaluated by transillumination ( Fig. 38.10E ). A segment of jejunum is selected and measured longer than the defect. Exact tailoring of flap length will be performed later during inset. The jejunal segment is centered on a proximal jejunal artery and vein of suitable diameter.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


