Product name
Substance
Organogen®
Paraffin-related substance
Bioplax®
Paraffin-related substance
DMPS®
Dimethylpolysiloxane
Ryn Sakurai’s serum®
DMPS plus animal or vegetable oil
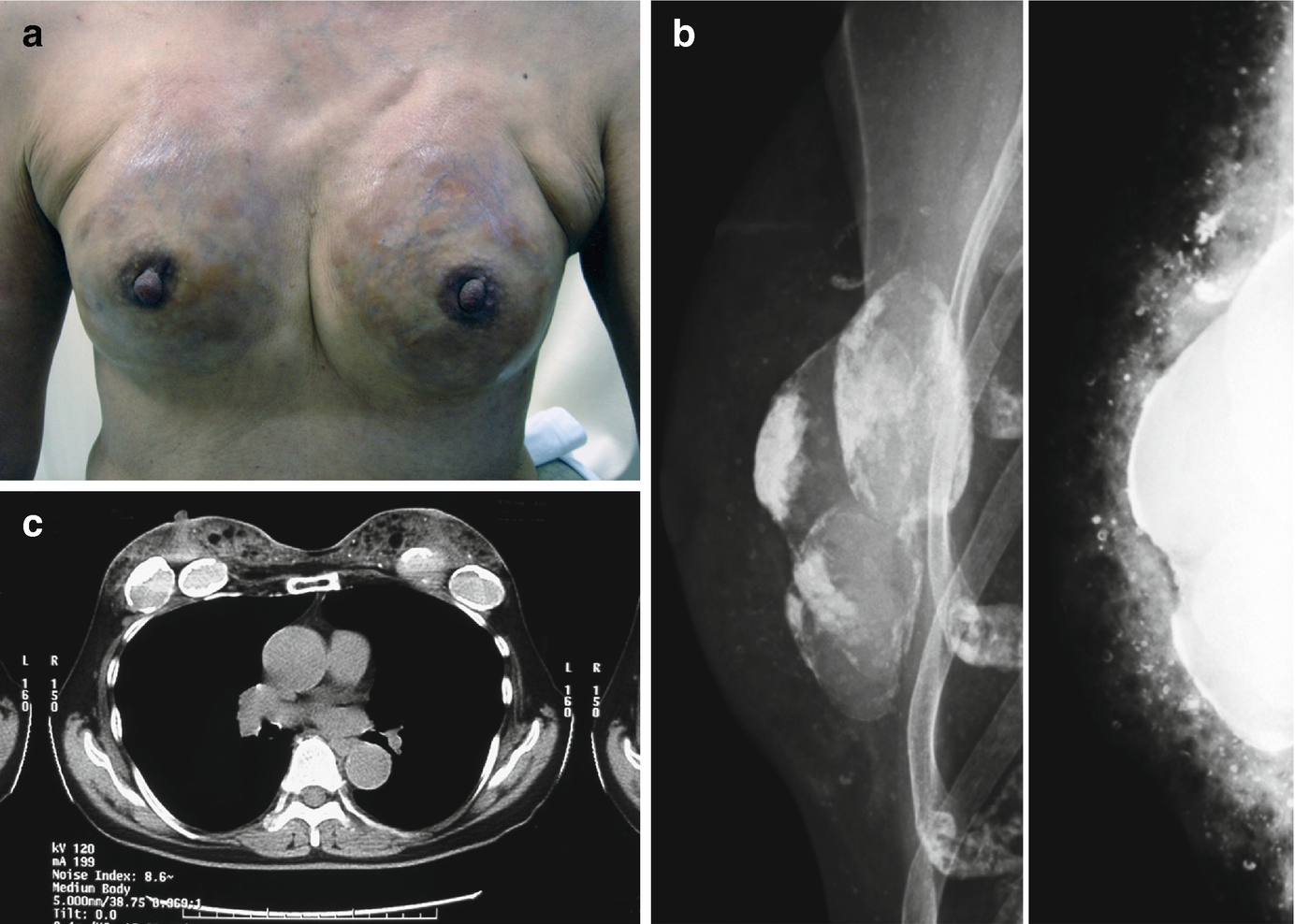
A rare case of breast augmentation with two different types of injectable materials. (a) The gross appearance of the patient. (b) The tungsten mammography image (left) and the molybdenum mammography image (right). (c) Computed tomography reveals the presence of radiopacity in the superficial layer and radiolucent structures with eggshell-like calcification in the deep layer
Local Symptoms of Breasts That Were Augmented by Injections with Artificial Injectable Materials
Several articles in the medical literature have documented the complications after breast augmentation with injectable materials in Japan and Western countries [9–12]. In most cases of complications, the injected material appeared to be silicone, as stated by the patient. However, it is possible that some of the cases in East Asian countries, including Japan, may have involved materials other than silicone and that this was not disclosed to the patient.
All patients with sequelae after breast augmentation with injectable materials had local complications. Different materials generally caused specific local complications. For example, since silicone generally stagnates in the injected area and tends not to spread out to the surrounding tissues, the main symptoms of silicone-injected breasts are subcutaneous indurations and relatively mild deformities. By contrast, hydrocarbon materials such as paraffin and “Organogen” spread easily from the injected site to the surrounding tissue, including the breast parenchyma, the pectoralis major muscle, and the skin. This can cause severe breast deformities, abnormal skin color and tone, and even ulceration of the skin. Moreover, these materials sometimes infiltrate the lymph nodes [11].
These clinical manifestations usually do not appear immediately after the injection. Subcutaneous induration or lump generally develops about a year after the injection and is the result of foreign body granuloma and chronic inflammation [13]. Ohtake et al. reported that the more disturbing symptoms most often arose 3–5 years after the injection. However, since some of their patients developed complications as long as 13 and 28 years later, they concluded that patients with sequelae from foreign material injection should continue to be followed up [6].
It remains unclear whether material injections into the breast parenchyma can cause breast cancer. Although many patients who underwent foreign material injection have developed clinical breast cancer [11, 14], several studies failed to detect a causative relationship between these injections and breast cancer [15–17]. However, the presence of a large subcutaneous hard nodule or mass due to foreign material injections could interfere with the early detection of breast cancer. Moreover, Japanese women may in general be reluctant to admit that they have undergone cosmetic procedures: this may cause them to hesitate to undergo breast cancer screening by mammography or ultrasonography, which could increase the risk of not detecting the cancer at an early stage. This notion is supported by the article of Ohtake et al., who found that 1.6% of their patients who underwent breast augmentation with injectable materials had breast cancer: this incidence is higher than the incidence of breast cancer in normal uninjected breasts [6].
Human Adjuvant Disease
In 1964, Miyoshi et al. reported two cases of connective tissue disease-like disorders in patients who had undergone breast augmentation with paraffin injection several years previously. One of these patients experienced a dramatic improvement in her disease symptoms after the foreign substances were removed by bilateral mastectomy. These experiences led Miyoshi et al. to suspect that the injected substance had an adjuvant property and that its prolonged presence had promoted the disorders in these patients. As a result, they proposed the term “human adjuvant disease” to describe the disorder [18].
Human adjuvant disease occurs after injection or implantation of paraffin/silicone and possibly silicone polymers. It can also occur after silicone migrates through a lymphatic or hematogenous pathway from the site of injection or implantation secondary to implant rupture or fragmentation [11, 19–23]. The signs, symptoms, and laboratory abnormalities of human adjuvant disease are suggestive but not diagnostic of a connective tissue or autoimmune disease [24]. The disease can be suspected when the following six characteristics are observed. First, the patient is a woman who developed autoimmune disease-like symptoms (including skin rash, joint pain, and Raynaud’s phenomenon) several years after plastic surgery with foreign substance injection. Second, the breasts or other areas of the body had been injected with paraffin, silicone, or related substances that might have adjuvant properties. Third, histopathology shows the presence of foreign body granulomas in the injected areas and their associated lymph node drainage systems. Fourth, the patient has serological abnormalities such as autoantibodies: Hyakusoku reported that approximately 25% of patients who undergo breast augmentation with injectable materials develop autoantibodies, including antinuclear antibody, anti-thyroglobulin antibody, anti-microsome antibody, anti-DNA antibody, and rheumatoid factor [25]. Fifth, the symptoms of the patient improve after the removal of the injected foreign substances. Sixth, the operated region lacks an infection or malignancy [26].
In 1980, a severe case of human adjuvant disease was reported by Fumiiri, who described the autopsy findings of a patient who underwent breast augmentation with injected materials and presented with subcutaneous induration, high fever, skin rash, lymphopenia, liver dysfunction, and hypergammaglobulinemia. The patient died 10 years after the procedure was performed, and the autopsy revealed the presence of the injected substance in not only the lymph nodes but also the liver and the bone marrow stroma [13].
Several articles have also shown that some women who undergo breast augmentation with injectable substitutes develop the diagnostic criteria of collagen diseases. When Kumagai et al. reviewed their 18 cases of collagen disease after breast augmentation with injectable materials plus another 28 cases in the Japanese literature, 24 patients were found to have definite connective tissue disease: 12 had scleroderma [of whom 8 had progressive systemic sclerosis (PSS)], 6 had rheumatoid arthritis, 5 had with systemic lupus erythematosus, and 1 had polymyositis [27]. In particular, the incidence of PSS in these 46 cases was higher than expected, and PSS was more likely to develop in patients who had been injected with paraffin. The remaining 22 cases had human adjuvant diseases with signs and symptoms that were suggestive but not diagnostic of a connective tissue disease.
Imaging Methods Used to Identify the Injected Materials
Summary of the imaging methods that can be used to identify the material that was injected for the purpose of breast augmentation
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


