(5.1)
where D i, c i, and u i are the diffusion coefficient, concentration, and electrical mobility of ion i and v w represents the linear velocity of the convective solvent flow (Gratieri and Kalia 2013). The diffusion coefficient and the electric mobility are related by the Nernst-Einstein equation:

(5.2)
Thus, the electric mobility represents an “ordered” diffusion dictated by the electric field – it competes against thermal disordering (RT term in the denominator) which will act to decrease its magnitude. It is clear that the higher the valence (z i), the higher is the electrical mobility. For charged molecules, passive diffusion across the stratum corneum is limited or negligible, meaning that molecular transport during iontophoresis is attributed to EM and EO – their relative contributions depending on the experimental conditions and the physicochemical properties of the molecule (Gratieri and Kalia 2013).
The penetration pathways of such charged molecules during iontophoresis may also be different from those during passive diffusion. Instead of following the tortuous intercellular lipid pathway between the corneocytes, it has been suggested that under the influence of an electric current, ions will follow the path of the least electrical resistance, e.g., they will preferentially take the appendageal pathways (i.e., hair follicles, sweat glands) (Cullander and Guy 1991). However, in addition to transport via these “shunt” pathways, structural changes in the membrane, which may correspond to transient reorientation of SC proteins and lipids in the presence of the electric field, may also facilitate ion transport (Jadoul et al. 1999). Lipids and proteins have dipole moments and will align themselves to the direction of the applied electric field. The reorientation of these SC components under the influence of the electric field may result in the formation of transient conduction pathways (“pores”) in the bulk SC (Gratieri and Kalia 2013). Therefore, although the appendageal structures are probably involved in iontophoretic transport, smaller negatively charged (given the skin’s permselectivity at physiological pH) transient “nano-pores” with estimated pore radii of ~20 nm may also be present (Aguilella et al. 1994) (Fig. 5.1).
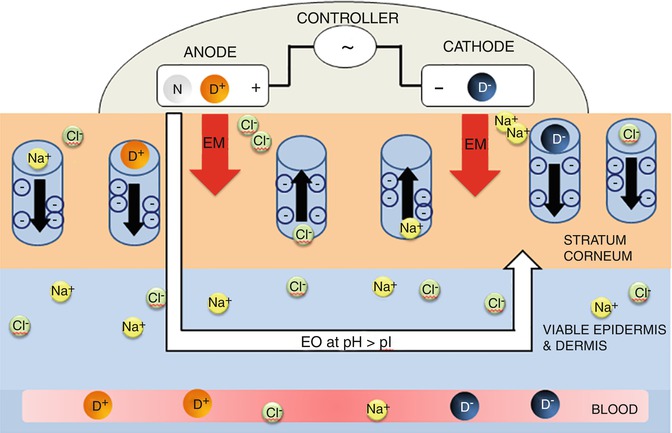
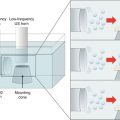
Fig. 5.1
Schematic representation of iontophoresis including the representation of transient pores created in the skin during current application. Under the influence of the applied field, it is envisaged that ions electromigrate through these pores – the presence of the fixed negative charges in the pore walls gives rise to electroosmotic phenomena (Pikal 1990). (Modified from (Gratieri and Kalia 2013). D is the drug, which can be either positively (D+) or negatively (D−) charged. N represents a neutral molecule. EM is the electromigration and EO the electroosmosis)
5.2 Factors Influencing Electrically Assisted Drug Delivery
5.2.1 Current Density
Electromigration refers to the ordered movement of the ions in the presence of the applied electric field in a process that can be described by Faraday’s law (Phipps et al. 1989; Phipps and Gyory 1992; Sage and Riviere 1992; Delgado-Charro and Guy 2001; Kalia et al. 2004):
where I is the applied current (amperes); t D is the transport number of the drug; A is the cross-sectional area through which transport occurs; F is the Faraday constant (Coulombs/mole); and z D is the drug valence.
(5.3)
It is evident from the equation that the applied current (I) is a parameter that can directly affect the rate and extent of drug delivery. The introduction of the second driving force – the electrical potential gradient – in addition to the concentration gradient across the skin (Gratieri and Kalia 2013), means that drug delivery is enhanced, and the flux can be strictly correlated with duration, intensity, and profile of current application. As such, complex drug delivery kinetics – determined solely by the current profile – are feasible. This was demonstrated in studies carried out in Yorkshire swine investigating the feasibility of delivering zolmitriptan (MW 287.4 Da) – used for the treatment of migraine. An iontophoretic patch system and a complex multistep current profile were used. The study showed that the drug levels in the blood (7.1 ± 1.7 and 11.9 ± 2.0 ng/ml at t = 30 and t = 40 min, respectively) closely followed the variations in the applied current (four-step profile with current intensities ranging from 0.35 to 0.05 mA/cm2) (Patel et al. 2009).
Many other studies have demonstrated that the iontophoretic flux of a drug can be enhanced by increasing the applied current (Green et al. 1992; Lau et al. 1994; Abla et al. 2005; Panzade et al. 2012); linear correlations between flux and current density have been reported either small molecules as thyrotropin (362 Da) (Burnette and Marrero 1986) or for larger molecules, e.g., triptorelin (1311.5 Da) (Schuetz et al. 2005). In this way, the modulation of the applied current and the patch size enables easy individualization of therapy (Djabri et al. 2012a). This was recently observed with rasagiline (RAS) and selegiline (SEL), which are dose-dependent selective irreversible inhibitors of monoamine oxidase B (MAO-B), with therapeutic applications for the treatment of Parkinson’s disease and in the treatment of major depressive disorder (Kalaria et al. 2012). Permeation experiments performed across porcine and human skin in vitro demonstrated that while passive delivery from aqueous solution was minimal, drug delivery was directly correlated with current density (I d = 0.15, 0.3, and 0.5 mA/cm2) producing a linear increase in steady-state iontophoretic flux (J ss, RAS = 49.1 I d + 27.9 (r 2 = 0.96) and J ss, SEL = 27.8 i d + 25.8 (r 2 = 0.98)). Drug extraction from the skin showed that there was also a statistically significant increase in the amounts of RAS and SEL retained within the membrane as a function of current density (Fig. 5.2).
Fig. 5.2
Total delivery (cumulative permeation + skin deposition) and steady state flux (Jtot) of (a) RAS (20 mM) and (b) SEL (20 mM) as a function of current density (at 0.15, 0.3, and 0.5 mA/cm2) across porcine skin after 7 h of transdermal iontophoresis (mean ± SD; n ≥ 5). (Adapted and reproduced with permission from Kalaria et al. 2012)
However, straightforward linear correlations are not always observed. For example, a poor correlation was observed between 9-desglycinamide-8-arginine-vasopressin (DGAVP) flux and applied current; a more than sixfold increment in current density did not even double the flux (Craanevanhinsberg et al. 1994).
It is also evident from Eq. 5.3 that a drug’s transport number influences the electromigration efficiency. This parameter is related to the ability of the drug to function as a charge carrier, and the transport number represents the fraction of the total charge carried by each species (0 < t D < 1) (Mudry et al. 2006a, b, c). It depends on how drug concentration, mobility, and valence compare with those of the other ions present in the pharmaceutical formulation (buffering agents, viscosity modifiers, and preservatives) generated by electrode reactions and present in the skin (Mudry et al. 2006a). Specifically,
where I d is the applied current density (= I/A) and z D, u D, and c D refer to the charge, mobility, and concentration of the drug in the membrane, respectively; the denominator is the sum of the products of these parameters for each ion in the system contributing to charge transfer across the membrane (Kalia et al. 2004; Kasting and Keister 1989). It is obvious that the presence of endogenous competing counterions decreases the iontophoretic transport of the drug.
(5.4)
5.2.2 Formulation
5.2.2.1 Drug Concentration
Drug concentration is a commonly studied experimental parameter in iontophoretic experiments, as it might be envisaged that an increase in the amount of drug in the formulation would result in increased drug delivery. However, linear correlations are not always encountered, and behavior is complicated by drug-membrane interactions. For certain molecules, the flux-concentration profiles reach a plateau above which further increases in concentration have only a limited or negligible effect on flux.
A key factor is the presence or absence of competing ions (Kasting and Keister 1989). Studies have described the use of a salt bridge to eliminate the presence of competing cations in the donor compartment rendering delivery independent of drug concentration. For example, it was observed that cumulative permeation of RAS after iontophoresis for 7 h using a salt bridge at 0.5 mA/cm2 was independent of drug concentration. For the three concentrations studied (10, 20 and 40 mM), the cumulative permeation was statistically equivalent (1200.4 ± 154.6, 1262.6 ± 125.0 and 1321.5 ± 335.2 μg/cm2, respectively); similar behavior was observed for SEL (the corresponding values were 748.3 ± 115.2, 848.8 ± 108.3, and 859.8 ± 230.1 μg/cm2, respectively) (Kalaria et al. 2012). Although the use of salt bridges precluded the presence of competing cations in the donor compartment, chloride ions present in the receptor were the principal charge carrier due to their high mobility and concentration as they migrated across the skin toward the anode – as would be the case in vivo (Kalaria et al. 2012).
In cases where a salt bridge is not used, Eq. 5.4 suggests that the increase of the drug concentration, or drug molar fraction, should enhance the transdermal flux via an increase in t D , therefore, increasing EM. This was recently demonstrated with the cathodal iontophoresis of phenobarbital in vitro across porcine skin. The results showed that drug fluxes were inversely related to the Cl– concentration present in the donor solution after 5 h of current application (0.5 mA/cm2) (Fig. 5.3a). Therefore, the lower the co-ion concentration, the greater the drug molar fraction in the vehicle and the greater the drug transport number in a linearly proportional manner (r 2 ≈ 0.80) (Fig. 5.3b) (Djabri et al. 2012b).
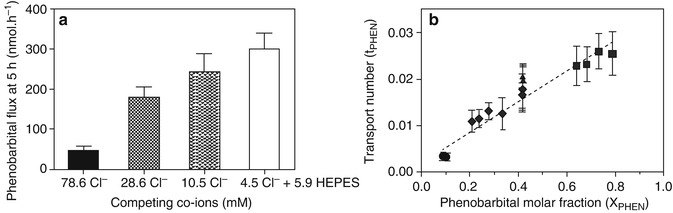
Fig. 5.3
Cathodal delivery of phenobarbital from different donor solutions (pH 7.4) containing various amounts of competing co-ions. (a) Flux values (mean ± SD) determined after 5 h of iontophoresis (0.4 mA). (b) Transport number of phenobarbital (t PHEN, mean ± SD) as a function of molar fraction (XPHEN). Values of the latter parameter were calculated from the concentrations of phenobarbital, HEPES, and chloride. The sources of Cl−included NaCl (used as background electrolyte), HCl (used to adjust the donor solution pH), and the electrode electrochemical reaction. The dashed line is the linear regression through all data points except those obtained with HEPES: t PHEN = 0.002 (±0.001) + 0.033 (±0.002) XPHEN (r 2 > 0.8). Adapted and reproduced with permission from Djabri et al. (2012b)
It may also be assumed that an increase in drug concentration would result in an increased EO flux, according to Eq. 5.5, which expresses the EO drug flux:

where v w is the electroosmotic solvent flow, and c D is the concentration of the drug in the vehicle (Pikal 1992). This should have a direct impact on the delivery of positively charged and neutral molecules. However, the real situation may be far more complex than the cited equations suggest, as other factors may be involved: not only the existence of competing ions, as mentioned before, but also the effect of drug physicochemical properties and their impact on the ability of the molecule to interact with structures along the iontophoretic transport pathway.
(5.5)
Studying the anodal iontophoresis of granisetron (GST; MW: 348.9, pKa 9.4) across porcine skin in vitro, it was demonstrated that cumulative delivery from 5 to 10 mM solutions was statistically equivalent; however, statistically significant increases were seen when drug concentration was raised to 20 or 40 mM (Cazares-Delgadillo et al. 2010). The reduced delivery efficiency at lower concentrations could be explained by the presence of Na+ in the formulation, which possesses higher mobility than granisetron, effectively negating the effect of any increase in formulation concentration (Kasting 1992). As the formulation pH (6.6–6.8) was higher than the skin’s pI, there was an EO contribution to delivery. However, co-iontophoresis of acetaminophen, a neutral molecule used to report on convective solvent flow, showed that EM was the predominant transport mechanism accounting for 71–86 % of total granisetron delivery. It was also observed that a fourfold increase in granisetron concentration from 10 to 40 mM resulted in a twofold reduction in acetaminophen permeation indicating that skin permselectivity was decreased (Cazares-Delgadillo et al. 2010). As for other lipophilic cations, including the peptides, leuprolide, and nafarelin, it is likely that the positively charged molecules were bound to skin structures along the iontophoretic transport pathway neutralizing the intrinsic negative charges, thereby reducing the volume of solvent flow (Lu et al. 1993; Delgado-Charro and Guy 1994; Hoogstraate et al. 1994; Delgado-Charro and Guy 1995; Delgado-Charro et al. 1995; Hirvonen et al. 1996; Rodriguez Bayon and Guy 1996; Hirvonen and Guy 1997; Nair and Panchagnula 2003). In these cases, the impact on drug delivery can depend on the relative contribution of EM and EO to the iontophoretic transport of the molecule in question (Hirvonen and Guy 1997; Marro et al. 2001b).
5.2.2.2 pH
In principle, the ionization state of the skin will determine the EO solvent flow, and in vitro studies have tried to use modification of formulation pH as a means to change skin pH. However, this is a strategy more suited to enhancing the ionization state of the drug and so affects mobility and hence EM, since manipulation of skin ionization state is rather more difficult to achieve in vivo due to the skin’s intrinsic buffering capacity (Levin and Maibach 2008). Although modulation of formulation pH can certainly be used to improve transport, in practice, extreme pH values need to be avoided to prevent irritation or chemical burns. Acceptable pH values for skin application have a mildly acidic to neutral pH (5–7.4).
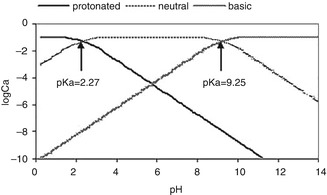
Acyclovir, for example, is an antiviral agent used in the treatment of cutaneous viral infections caused by herpes simplex virus (HSV-1). Although it is a small molecule (225.20 Da), it is unable to diffuse efficiently through the SC and subsequently enter into the basal epidermis, where viral replication occurs. In order to enhance the permeation of this molecule, iontophoresis has been applied by many authors (Volpato et al. 1995; Volpato et al. 1998; de Jalon et al. 2001; Stagni et al. 2004; Padula et al. 2005; Morrel et al. 2006; Shukla et al. 2009; Siddoju et al. 2011). However, it has been shown that at pH 7.4, the amount of drug recovered in the stratum corneum and epidermis after iontophoresis was similar to that obtained after passive diffusion (Volpato et al. 1998). This is because acyclovir is essentially uncharged at physiological pH (pKa1 2.27; pKa2 9.25); hence EO is the only enhancing mechanism. However, even delivery by EO is compromised due to its low aqueous solubility (1.3 mg/ml at pH 7.4, 25 °C). For this reason, other studies employed formulations with extreme pH to have the drug molecule in an ionized state (Fig. 5.4). For example, after 10 min cathodal iontophoresis of acyclovir gel at pH 11 to hairless rats in vivo, fourfold more ACV was detected in the SC as compared with passive delivery (30.70 ± 4.83 and 7.83 ± 1.59 μg/cm2, respectively) (Siddoju et al. 2011). Improved delivery to the dermis was observed in rabbits in vivo after 1 h of cathodal iontophoresis at pH 11 (Shukla et al. 2009). However, although the authors reported there were no additional signs of skin irritation on the conditions used, it is rather implausible that a formulation with such an irritant pH can be of practical use.
 Iontophoresis: Basic Principles
Iontophoresis: Basic Principles
 Microporation in Penetration Enhancement
Microporation in Penetration Enhancement
 Combined Use of Ultrasound and Other Physical Methods of Skin Penetration Enhancement
Combined Use of Ultrasound and Other Physical Methods of Skin Penetration Enhancement
 Gene Transfer to the Skin by Physical Methods of Delivery
Gene Transfer to the Skin by Physical Methods of Delivery
 Electroporation for Dermal and Transdermal Drug Delivery
Electroporation for Dermal and Transdermal Drug Delivery
 Therapeutic Applications of Electroporation
Therapeutic Applications of Electroporation




Related posts:
Microporation in Penetration Enhancement
Combined Use of Ultrasound and Other Physical Methods of Skin Penetration Enhancement
Gene Transfer to the Skin by Physical Methods of Delivery
Electroporation for Dermal and Transdermal Drug Delivery
Therapeutic Applications of Electroporation
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
