General Principles
Avoidance and management of complications begins prior to making the first incision. “Extreme ownership,” initially coined by Navy SEAL Jocko Willink, is a concept in leadership that defines a true leader as an individual who takes responsibility of not just their own actions and behaviors, but also the people and the environment around them. A successful surgeon must embody this notion of leadership, taking ownership of both the positive outcomes of the procedure and the negative outcomes and possible complications. 1 A true surgeon understands that the negative outcomes of a surgical procedure cannot be attributed to a patient’s level of compliance or shortcomings, anesthesia care, or factors “outside their control.” But instead, he or she takes responsibility as the surgeon and accepts negative outcomes with self critique, such as being due to a lack of maturity and/or attention to detail. Success is dependent on the surgeon’s ability to be self-aware and cognizant of all the variables influencing his patients care, all the while evaluating his own standards of care for quality improvement. He must practice “extreme ownership” in order to ensure patient-centered care throughout the entirety of the clinician–patient interaction from preoperative assessment to postoperative care. Although seemingly impossible, maintaining this mindset and developing a practice around these principles will, without question, improve the doctor–patient relationship, improve outcomes, and ultimately lead to a reduction in complication rates. It entirely becomes the surgeon’s responsibility to reduce rates of complications and substandard results, and in doing this, there are no longer factors outside the surgeon’s control given these factors will have been foreseen and optimized for surgery from the beginning.
Effective conduct of the operation begins with very accurate patient assessment in conjunction with the anesthesia provider and accurate assessment of what the patient is able to contribute to his own care. This includes not just the patient’s health, but also their ability to understand the operative process and to comply with postoperative instructions including even simple social issues such as transportation or home nursing issues.
Optimizing the next steps in the operative process, including anesthesia and supplies, comes with repetition and attention to detail. Dedicated anesthesia staff, dedicated surgical instruments, and disposables eliminate variability and distractions.
Properly done, the only variables become the patient and their Mohs defects, and operating can become a seamless “flow state” that is both safe and enjoyable for all involved.
20.1.1 A Note on Patient Consent
Undertaking a complex multistage Mohs repair is somewhat similar to accompanying the patient on a journey through a hostile land. The surgeon can serve as the experienced guide and prevent pitfalls along the journey to a successful repair.
The consent process should not be an opportunity to discuss every possible outcome and it is foolish of a surgeon to discuss fatalities from an operative procedure for Mohs repair. Yes, fatalities can result, but one does not sign an equivalent consent on fatalities from a domestic airline flight when the safety rate for both are very similar. 2 It is unnerving for the patient and legally unnecessary. It is incumbent upon the surgeon to discuss possible adverse outcomes and briefly consider all options including doing nothing. The first or second postoperative visit is also an ideal time to discuss long-term outcomes with regard to finer results and to discuss in much greater detail the need for possible revisions. At this time, it is also an opportunity to review the procedure performed in depth and with the use of postoperative photos, discuss the initial appearance, that is, where we are now and what the expected outcome is, as well as the time course of this surgery. Patients will find this very reassuring and in many cases they can make travel and work plans based on the physician’s illustration. Understand that the patient, on the initial postoperative visit, is looking up to the doctor for “how they are supposed to look” and oftentimes they consider the physician as a guide on an extended journey or travel toward their final outcome.
20.2 Intraoperative Complications
Summary
Intraoperative complications experienced in Mohs repair have included fire, bronchospasm, preoperative anaphylaxis, eye injuries, and nerve injuries.
20.2.1 Fire
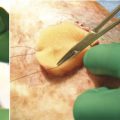
Unfortunately, the incidence of intraoperative fire is not zero. It is an entirely avoidable event. The use of awake intravenous (IV) sedation, which provides multiple benefits to the patient, is often accompanied by the concurrent use of oxygen by nasal cannula and if inappropriately managed, it can lead to flash fires on the table. The current standards on oxygen administration—during the use of Bovie cautery—is to simply not use oxygen at no greater than 30% FiO2 at all during the case. 3, 4 If patient conditions mandate higher oxygen concentrations, then very accurate communication between the surgeon and the anesthesiologist allows for its safe effective use. Consistent draping with four towel drapes where the entire head is left exposed and no tenting for possible oxygen containment is mandatory, and the removal of the Bovie tip while the oxygen is in use will prevent the inadvertent ignition source. The removal of all surgical prep solution is mandatory as well as ensuring availability of damp surgical laps on the surgical field (▶ Fig. 20.1 and ▶ Fig. 20.2).

Fig. 20.1 A 62-year-old male with nasal sidewall defect repaired by single-stage island nasolabial flap. Repair complicated with intraoperative fire from electrocautery igniting oxygen delivered by nasal cannula. Wounds healed without long-term sequelae. Incident resulted in policy change of discontinuing oxygen delivery by nasal cannula during intravenous anesthetic sedation.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


