Cutaneous squamous cell carcinomas (SCCs) account for up to 10,000 deaths annually in the United States. Most of the more than 700,000 SCCs diagnosed are cured by excision with clear margins; however, metastasis can occur despite seemingly adequate treatment in some cases. Immune-suppressed organ transplant recipients are 60 to 100 times more likely to develop SCC than immune-competent individuals. Transplant-associated SCCs occur more frequently and behave more aggressively, showing higher risk of recurrence and metastasis. This article identifies a potential role for interleukin-22 in driving SCC proliferation, particularly in solid organ transplant recipients taking cyclosporine.
Key points
- •
Cutaneous squamous cell carcinoma (SCC) is frequently curable, but causes significant morbidity and mortality, particularly in immune-suppressed organ transplant recipients.
- •
The SCC tumor microenvironment is rich and composed of multiple subsets of immune cells that exert antitumor and protumor effects.
- •
Interleukin (IL)-22 and its receptor are highly expressed in SCC and more so in transplant-associated SCC.
- •
IL-22 mediates SCC proliferation; an effect that is potentiated by cyclosporine.
- •
IL-22 blockade results in decreased SCC burden in a murine model system in vivo and may represent a therapeutic target.
| AK | Actinic keratosis |
| APC | Antigen-presenting cell |
| CSA | Cyclosporine A |
| DC | Dendritic cells |
| IL | Interleukin |
| iNOS | Inducible nitric oxide synthase |
| LC | Langerhans cell |
| mTOR | AKT-mammalian target of rapamycin |
| NFAT | Nuclear factor of activated T cells |
| NK | Natural killer cell |
| OTR | Organ transplant recipient |
| MMP | Matrix metalloproteinase |
| SCC | Squamous cell carcinoma |
| STAT | Signal transduced and activator of transcription |
| TAM | Tumor-associated macrophage |
| TNF | Tumor necrosis factor |
| Treg | Regulatory T cell |
| TSCC | Transplant-associated squamous cell carcinoma |
| VEGF | Vascular endothelial growth factor |
Introduction
Cutaneous squamous cell carcinoma (SCC) is the second most common human malignancy, with more than 700,000 cases expected in 2016. Although typically curable by excision with clear margins, SCC can behave aggressively and metastasize to local lymph nodes despite treatment. Cutaneous SCC is characterized by the malignant proliferation of keratinocytes that typically occurs on sun-damaged skin and tends to develop within areas of noninvasive actinic keratosis (AK). Progression from AK to SCC is thought to occur as a result of ultraviolet (UV)-induced mutations in proto-oncogene genes, with as few as 2 mutations being sufficient to drive SCC development. Additional factors from the tumor microenvironment likely influence SCC progression.
Introduction
Cutaneous squamous cell carcinoma (SCC) is the second most common human malignancy, with more than 700,000 cases expected in 2016. Although typically curable by excision with clear margins, SCC can behave aggressively and metastasize to local lymph nodes despite treatment. Cutaneous SCC is characterized by the malignant proliferation of keratinocytes that typically occurs on sun-damaged skin and tends to develop within areas of noninvasive actinic keratosis (AK). Progression from AK to SCC is thought to occur as a result of ultraviolet (UV)-induced mutations in proto-oncogene genes, with as few as 2 mutations being sufficient to drive SCC development. Additional factors from the tumor microenvironment likely influence SCC progression.
The tumor microenvironment of squamous cell carcinoma
Gene expression profiling of invasive SCC has revealed the presence of a large inflammatory response. On a broad level, immune cells are thought to play a role in the antitumor response. These immune cells include Langerhans cells (LCs), dermal dendritic cells (DCs), CD4+ and CD8+ T cells, T regulatory cells (Treg), macrophages, and natural killer (NK) cells. For SCC, some cell types typically implicated in tumor eradication, NK, B cells, and monocytes, are rarely detected surrounding and infiltrating tumors. However, CD4+ and CD8+ T cells, DCs, and tumor-associated macrophages (TAMs) are often found infiltrating SCC tumors ( Fig. 1 ). These cells are thought to stunt malignancy and promote regression of primary tumors, but in the context of SCC some of these cell types may be functionally impaired or may exert protumor effects.
T cells are a significant component of the SCC microenvironment. Gene expression profiling has shown that T-cell activity is decreased in SCC, as shown by downregulation of activation maker CD69 and impaired secretion of granzyme B and inducible nitric oxide synthase (iNOS). In addition, myeloid-derived suppressor cells are present in SCC and function to impair T cell–mediated immunity by secreting nitric oxide in the tumor microenvironment. The consequence of this is dampening E-selectin expression on epithelial cells and impairment of T-cell entry into tumors. In contrast, human T cells have been reported to secrete interleukin (IL)-24 in response to antigen stimulation, secretion of which has been shown to increase matrix metalloproteinase (MMP)-7 gene expression by SCC cells in culture, potentially contributing to SCC invasion. Antibody blocking of SCC cells with MMP-7–specific antibody has been shown to significantly delay SCC migration.
Antigen-presenting cells (APCs) in the skin include epidermal LCs and dermal myeloid DCs. Myeloid DCs from SCC do not stimulate T-cell proliferation, even when cultured in the presence of maturation promoting cytokines such as IL-1β, IL-6, tumor necrosis factor alpha (TNFα) and prostaglandin E2. These data might indicate a significant gap in defense against SCC. This possibility is further supported by the presence of IL-10 and transforming growth factor beta (TGFβ) in the SCC microenvironment and expression of CD200 receptor by SCC-associated DCs. Each of these has been shown to decrease DC-mediated T-cell responses. LCs, located in the epidermal layer, should be the first APCs to encounter SCC tumor antigens generated by transformed keratinocytes. These cells are primarily found in tissues adjacent to and including the interface with the tumor. Moreover, LCs from SCC have been shown to stimulate CD4+ and CD8+ T-cell proliferation at rates higher than those from normal skin eliciting a type 1 T-cell response. In addition, they express higher levels of LC maturation markers, CD40, CD80, CD83, and CD86. This finding might indicate an antitumor role for LCs in human SCC. In contrast, diphtheria toxin depletion of LCs in mice decreases ultraviolet B (UVB)–induced SCC tumor growth. These data suggest that LC responses somehow contribute to SCC tumor growth. LCs from SCC have been reported to express immune-activating signal transducer and activator of transcription (STAT) 4, IL-15, and CD80, and immune tolerizing CD200 genes. Therefore, it is possible that LCs can have protumor roles in the context of SCC, despite their ability to elicit T-cell responses.
An abundance of TAMs are found surrounding as well as penetrating SCC. TAMs may play a dual role in the tumor microenvironment, because they maintain the potential to eradicate tumor cells but have been shown to promote tumor growth. TAMs in the SCC microenvironment have been shown to be classically activated M1 marker, alternatively activated M2 marker, or biactivated M1 and M2 marker expressing ( Fig. 2 ). M1 activation is driven through the type 1 T helper (Th1) cytokine interferon gamma (IFNγ), whereas M2 activation occurs as a result of type 2 T helper (Th2) cytokines, which include IL-10, IL-13, and IL-4. Although M1 macrophage responses are thought to prevent tumor growth, the predominant subtype found in SCC tumors are M2 macrophages, which have lower antigen-processing capacity. In addition, they have been shown to negatively correlate with tumor growth and progression. The authors found that SCC TAMs express MMP-11, MMP-9, STAT1, STAT6, and vascular endothelial growth factor C (VEGF-C), which have been shown to promote increased lymphatic vessel density that is correlated with increased metastasis. Hence, SCC TAMs may show poor antigen-presentation capacity in addition to secreting factors that may potentiate tumor progression.
Transplant-associated squamous cell carcinoma
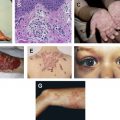
Solid organ transplant recipients (OTRs) represent a particularly high-risk population for the development of SCC. Immunosuppressive therapy used by OTRs to prevent allograft rejection predisposes patients to cutaneous infections and neoplasms. OTRs are 60 to 100 times more likely to develop transplant-associated SCC (TSCC) compared with age-matched immune-competent populations. Patients with TSCC may experience catastrophic body surface area involvement with metastatic rates as high as 8% ( Fig. 3 ).
Similar to SCC in immune-competent patients, TSCC tumors were shown to have heightened levels of inflammatory gene expression measured using gene set enrichment analysis. More recently, the authors showed that TSCC tumors contain a higher percentage of IL-22–producing CD8+ T cells and increased expression of the IL-22 receptor. IL-22 has been shown to promote SCC proliferation in a dose-dependent manner in vitro. In addition, IL-22 drives inflammation and suppresses keratinocyte apoptosis; this may explain the increased proliferation and poorer outcomes observed in patients with TSCC.
General overview of interleukin-22 signaling
Interleukin (IL) 22 is a cytokine that was discovered in 2000 after being cloned from activated T cells. IL-22 targets cell types comprising outer-body barriers such as respiratory and intestinal epithelial cells, hepatocytes, and keratinocytes, but not cells of hematopoietic origin. The cytokine plays an important role in tissue homeostasis, tissue repair, and wound healing. Moreover, its expression has been linked to the development and progression of multiple carcinomas.
IL-22 is characterized as an IL-10 cytokine family member along with IL-10, IL-20, IL-24, and IL-26. The cytokine signals via the heterodimeric transmembrane IL22 receptor (IL-22R) 1 and IL-10R2, and shares IL-22R1 with 2 other IL-10 family members, IL-20 and IL-24. Signaling through the IL-22 receptor primarily induces Janus kinase activity and STAT transcription factors. In primary cells, STAT3 activation is the main event observed, along with weak activation of STAT1 and/or STAT5. In addition, activation of mitogen-activated protein kinase (MAPK), phosphoinositide 3-kinase (PI3K), and AKT–mammalian target of rapamycin (mTOR) also occurs.
The cellular sources of IL-22 are CD4+ T cells (Th17, Th22), CD8+ T cells (Tc17, Tc22), γδ T cells, NK T cells, and lymphoid tissue inducer cells. Although a wide variety of innate and adaptive cell types have been shown to secrete IL-22, CD4+ T cells (Th17 and Th22) and innate lymphoid cells are considered the predominant source of IL-22 in humans. As mentioned earlier, CD4+ and CD8+ T cells, often found infiltrating tumors, play an important role in SCC progression.
Role of interleukin-22 in squamous cell carcinoma
The role of IL-22 in skin cancer is an area of active research. It was reported that cutaneous SCCs contain high numbers of infiltrating IL-22–producing CD4+ T cells, whose recruitment to the tumor partially depended on matrix metalloproteinase 10 (MMP-10) and S100A15 production. The authors found IL-22, IL-22R, and downstream mediator phosphorylated STAT3 (pSTAT3) to be highly expressed in SCC ( Fig. 4 ). Further, IL-22 treatment of SCC results in enhanced proliferation in vitro ( Fig. 5 ). IL-22 has been shown to increase iNOS expression and activity, contributing to proinflammatory as well as proangiogenic properties in colon carcinoma cells. In SCC, iNOS expression has been reported and correlates with enhanced tumorigenic potential. SCC-associated DCs contain a subset of TNFα-positive, iNOS-positive cells. Dermal keratinocyte iNOS expression is enhanced by UVB irradiation, which is an environmental factor linked to SCC development. Further studies are necessary to determine whether IL-22 treatment coupled with UVB irradiation could promote increased SCC tumor growth as a result of iNOS expression. Importantly, administration of IL-22 antibody to SKH-1 animals during UVB-induced cutaneous carcinoma resulted in a decrease in the number and size of SCC tumors. This result further confirms the role of IL-22 in promoting SCC tumorigenesis.
Related posts:
 Basic Science Insights into Clinical Puzzles
Basic Science Insights into Clinical Puzzles
 Establishing Tolerance to Commensal Skin Bacteria
Establishing Tolerance to Commensal Skin Bacteria
 Dermatologic Manifestations of Monogenic Autoinflammatory Diseases
Understanding Inherited Cylindromas
Dermatologic Manifestations of Monogenic Autoinflammatory Diseases
Understanding Inherited Cylindromas
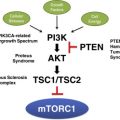 Mosaic Disorders of the PI3K/PTEN/AKT/TSC/mTORC1 Signaling Pathway
Mosaic Disorders of the PI3K/PTEN/AKT/TSC/mTORC1 Signaling Pathway
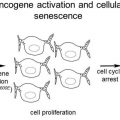 Melanocytic Nevi and the Genetic and Epigenetic Control of Oncogene-Induced Senescence
Melanocytic Nevi and the Genetic and Epigenetic Control of Oncogene-Induced Senescence
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


