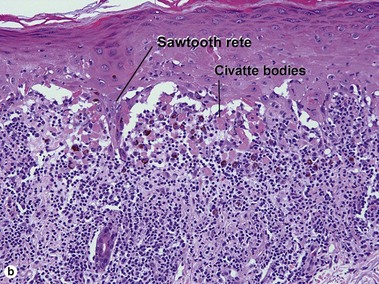
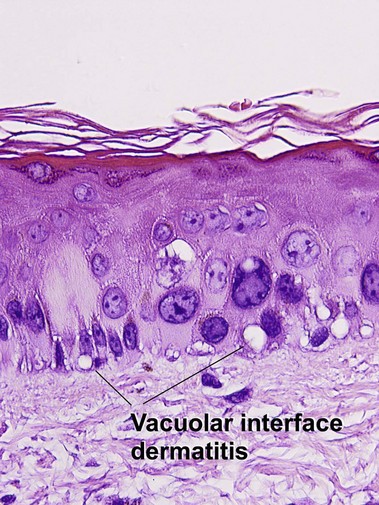
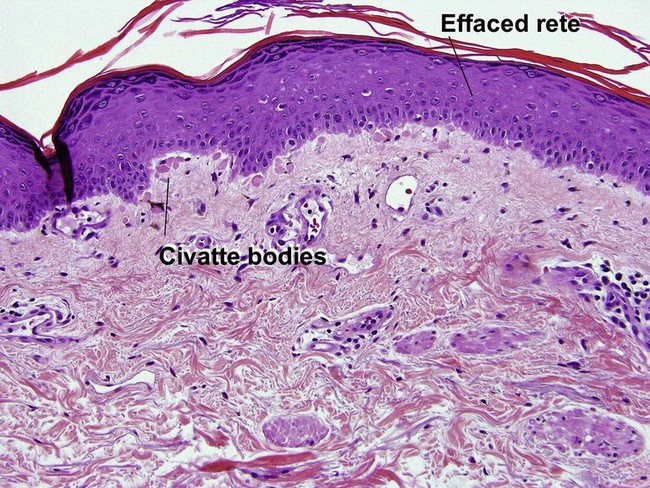
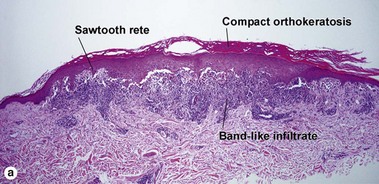
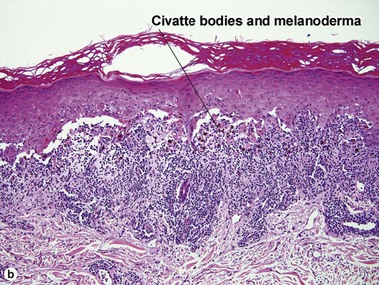
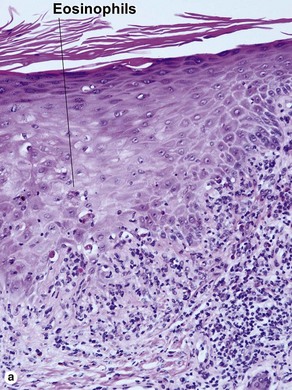
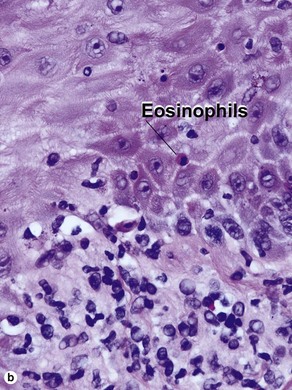
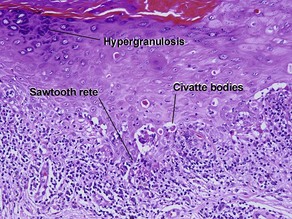
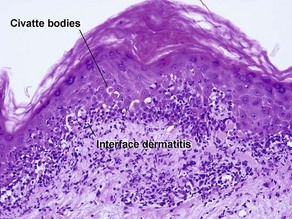
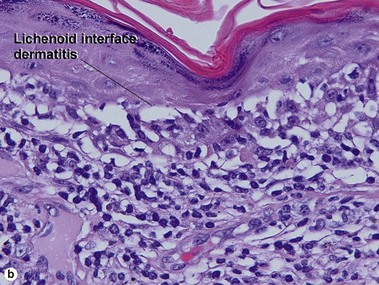
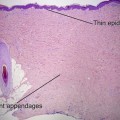
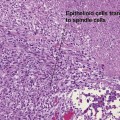
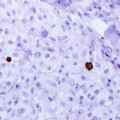
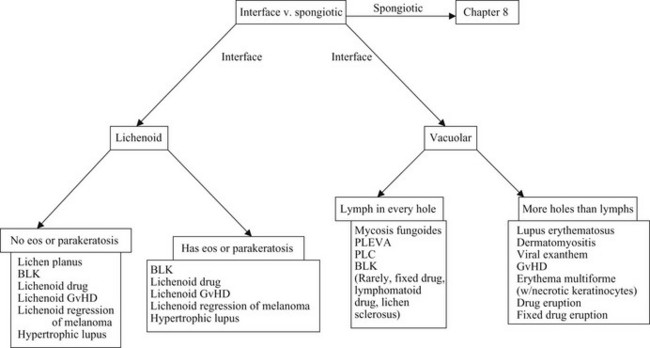
Chapter 7 • Benign lichenoid keratosis (BLK, lichen planus-like keratosis) • Lichenoid graft-versus-host disease (GvHD) • Hypertrophic lupus erythematosus • Lichenoid regression of a melanocytic lesion (usually lentigo maligna) The biopsy in each of these conditions demonstrates a sawtooth rete ridge pattern with destruction of the basal layer, a band-like lymphoid infiltrate, and presence of Civatte bodies. Compact hyperkeratosis and beaded hypergranulosis are typically present. The cells of the stratum spinosum are enlarged and more eosinophilic than the normal epidermis. Vacuoles may be present in the lowest cells of stratum spinosum, but the basal layer is gone. An underlying band-like lymphoid infiltrate is common. Fig 7-1 Interface versus spongiotic dermatitis (eos, eosinophils; PLEVA, pityriasis lichenoides et varioformis acuta; PLC, pleomorphic lobular carcinoma)
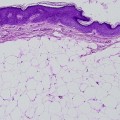
Interface dermatitis
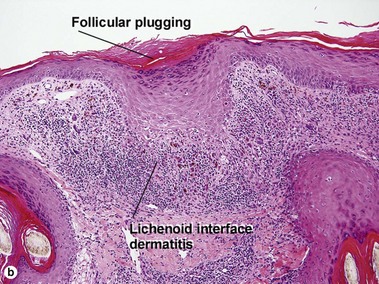
Lichenoid interface dermatitis
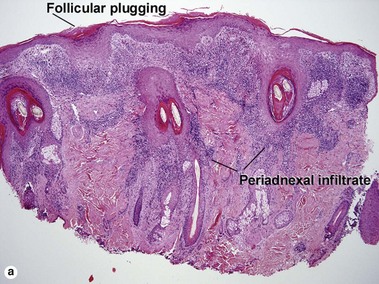
Causes of lichenoid interface dermatitis
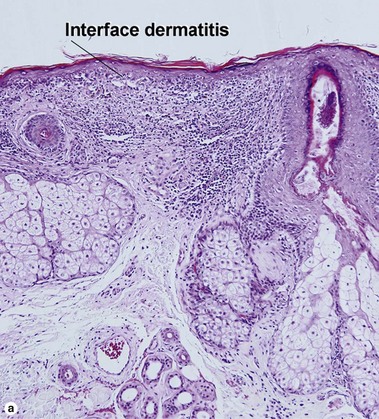
Interface dermatitis