Multiple fillers are available: various hyaluronic acid products, calcium hydroxylapatite, and a few others that are biocompatible with good duration and a variety of mechanical properties allowing intradermal, subdermal, and supraperiosteal injection. Facial features can be reshaped with great control using these fillers. Aging changes, including facial volume loss, can be well-corrected. These treatments have become a mainstay of rejuvenation in the early facial aging patient. Injection technique is critical to obtaining excellent results. Threading, fanning, cross-hatching, bleb, and pillar techniques must be mastered. Technical execution can only measure up to, but not exceed, the quality of the aesthetic analysis.
Key points
- •
Fillers are selected based on the biophysical properties for the tissue depth and type of correction contemplated.
- •
Fillers can restore facial volume aging loss or change the shape of the face.
- •
A combination of injection techniques usually produces a more complete correction.
- •
Correction of all of the deficits in a given region produces a more complete and harmonious correction than treating isolated features.
Introduction
Injectable fillers have become a prominent part of modern facial rejuvenation with more than 1.9 million treatments a year in the United States. This growing popularity has been fueled by the advent of multiple biocompatible and reasonably durable filler materials, most notably hyaluronic acid (HA) fillers, allowing a number of previously unmet needs to be addressed in a predictable and reproducible manner. Treatment of facial volume loss owing to aging is the most common application, correcting a variety of early and late changes. The immediacy, predictability, and safety of these no-downtime treatments make them the treatment of choice in most clinical circumstances. By adding volume or shape restoration of the aging face, in combination with energy-based treatments (lasers, radiofrequency, and others) for skin surface changes, such as wrinkles and pigmentary changes, and surgical lifting for skin laxity, a more complete correction of the aging face can be obtained.
Introduction
Injectable fillers have become a prominent part of modern facial rejuvenation with more than 1.9 million treatments a year in the United States. This growing popularity has been fueled by the advent of multiple biocompatible and reasonably durable filler materials, most notably hyaluronic acid (HA) fillers, allowing a number of previously unmet needs to be addressed in a predictable and reproducible manner. Treatment of facial volume loss owing to aging is the most common application, correcting a variety of early and late changes. The immediacy, predictability, and safety of these no-downtime treatments make them the treatment of choice in most clinical circumstances. By adding volume or shape restoration of the aging face, in combination with energy-based treatments (lasers, radiofrequency, and others) for skin surface changes, such as wrinkles and pigmentary changes, and surgical lifting for skin laxity, a more complete correction of the aging face can be obtained.
General approach
Detailed knowledge of facial anatomy, typical aging changes in the face, and aesthetic planning are essential to obtain artistic, balanced, natural-looking results. Filler injection is extremely technique dependent. Basically, a 3-dimensional latticework of injected material is being placed beneath the skin surface to add volume, change surface conformation, or thicken skin or subcutaneous tissues or fill a rhytid. All of these things are a form of sculpture, which result in a change in facial appearance. The degree of correction and the volume required for any given result is greatly dependent on the injection technique used. Likewise, pushing beyond the limits of what the treatments can reasonably produce is a sure recipe for unnatural looking results, or worse, tissue damage and complications. As benign as these treatments are in most cases, even after repetitive treatments, excessive volume or frequency of treatment is likely to result in trouble that is otherwise easily avoided.
There are many specific details to treating each anatomic area of the face. However, there are certain overall principles that apply in all these areas. First, no one filler is the correct choice for any application. Next, no one filler is going to be optimal for all the application areas in routine clinical practice. Each provider must select at least a small number of fillers to stock and needs to become facile at the specific feel and nuances of those fillers.
Choice of filler
As stated, no one filler is the correct choice for any application. Like selecting a golf club for a particular shot, a few clubs may be workable in skillful hands. Clearly, some choices will not work in a given situation (eg, a very soft, spreadable filler will not create a sharp, sculpted shape in the cheeks). The starting place for filler selection in this author’s hands relates to the anticipated depth of placement. Subcutaneous or supraperiosteal (but an exception is in the orbital area) fillers are generally heavier, which means higher viscosity and cohesivity. Fillers such as calcium hydroxylapatite (CaHa) and high-viscosity, high-cohesivity HA fall into this category. The original lower viscosity HA fillers work well in the deep dermal tissue plane or at the dermal/subcutaneous junction. Thinner fillers (which have lower viscosity and elastic modulus) such as monophasic, polydensified HA are suitable for middermal injection. The circumstances most appropriate for a given depth of injection are illustrated in detail in the specific anatomic application areas discussed elsewhere in this article.
At the time of this writing, the filler selection approved by the US Food and Drug Administration (FDA) for aesthetic use is a relatively short list. With the introduction of multiple new fillers to the marketplace, filler selection will necessarily change. Such selection is guided by the general principles discussed herein, clinical experience, and performance of the new product as determined by the community of clinical providers after several years of use and the filler alternatives available at that particular time. The techniques and selection presented herein represent this author’s preferred or usual techniques, but certainly not the only or necessarily best option. Each physician must base clinical choices on what works best in his or her hands.
Although neocollagenesis secondary to a pressure phenomenon inducing collagen synthesis in fibroblasts has been demonstrated secondary to HA filler injection, the magnitude of collagen replacement attributable to this mechanism is unclear. Nonetheless, recurrent treatment with HA fillers seems to provide longer intervals and reduced volumes after several treatments, suggesting that there is clinical significance to these findings.
It is not necessary to stock all HA fillers. Wide cross-applicability exists; however, this author believes that the fine features of each filler provide nuance to the correction that make them preferable for certain treatments. Other injectors might prefer a different filler.
CaHa particles stimulate neocollagenesis through an inflammatory-mediated mechanism that produces significant collagen to replace the gel carrier which absorbs over the first 3 to 4 months. This is a unique combination of time zero contour improvement followed by neocollagenesis. The filler also has mechanical properties that are unique, providing a high elastic modulus compared with other available products. The safety profile and tolerance of the material is excellent even after recurrent use of significant volumes. Owing to the time zero correction, a close match between what you see during treatment and what you get in clinical correction—stiffer mechanical properties and greater longevity—this filler is well-suited where defined shapes or sculpting are needed.
This author has restricted clinical practice to using only biological fillers with FDA approval for an aesthetic facial indication. Nonbiological, nonabsorbable materials in soft tissue locations have had a troubled past. Owing to the permanent nature of many of these materials, the potential for late misadventure is concerning. Breakdown of the materials after protracted residence in the body is another issue that will only manifest many years after adoption of a new material. Concern regarding biofilm formation on such materials is also a factor. Given the appropriately low tolerance of providers and patients for complications with aesthetic treatments, the biological, absorbable options seem preferable, particularly given the increased filler volumes and treatment frequencies that are being used. Whether a nonbiological nonabsorbable filler that is biocompatible and safe over the long term will be developed in the near future remains to be seen.
Because the details of differences in cross-linking and physical structure between different HA fillers is discussed elsewhere in this volume, this article does not reiterate these facts, but summarizes by saying that these differences affect physical properties, which in turn affect the clinical performance of the fillers. Clearly, as more fillers enter the marketplace, a careful understanding of multiple physical properties of the fillers is going to be increasingly important to aid in filler selection.
The details presented herein represent this author’s preferred injection techniques as a snapshot at the time of this writing. Other injection techniques might perform just as well and different techniques might be useful in an individual patient. The introduction of new fillers will change this perspective continuously, both in terms of inclusion of new filler options and the optimal techniques for injecting them.
Facial rejuvenation with fillers: volume restoration
Volume restoration of the aging face has become the most commonplace mainstay of medical facial rejuvenation. The face begins losing fat start some time in the late 30s. This produces a change in facial shape with blunting of the prominence and width of the malar eminence, loss of definition of the angle of the jaw, and descent of the cheek fat pads. Not only is the face losing fat, but fat pads in the face are either descending and/or losing volume at different rates, creating visible segmenting of facial compartments that seemed to be confluent in youth. These changes, along with loss of skin elasticity and development of skin laxity, result in progressive deepening of folds and creases in the face. The primary treatment for such changes, particularly early in the aging process, is with injectable fillers.
Liquid facelift: the role of volumization in skin laxity
With a patient population that is increasingly averse to operative procedures and anxious to minimize or even avoid recovery time, providers have added volume in the form of off-the-shelf fillers to take up some of the slack in lax facial skin. This is particularly helpful in the cheek, jowl, and nasolabial areas and to some extent in the brow and upper eyelid. The neck is not amenable to a decrease in laxity using injectable fillers. Because the face loses volume during aging, some measure of volume restoration has a good biological rationale, in addition to the practical dimension. For early facial aging, or a small degree of contour improvement, injectable fillers work quite well. Fat grafting is an alternative, albeit one with a trip to the operating room and at least some recovery time.
For patients with moderate or advanced skin laxity, fillers do not provide a meaningful option because the amount of volume required is both cost prohibitive and will leave the patient looking overplumped which is not a desirable aesthetic enhancement, even if less skin laxity is apparent. As in all treatment decision making, staying within the boundaries of a natural appearance shows us where to draw the line and move on to a bigger intervention, like surgical lifting.
Changing facial features with filler
Many facial features can be altered modestly to moderately using injectable fillers in either the aging patient or the youthful patient. Filler injections in the cheeks, chin, nose, brows, and angle of the jaw can create a change in facial shape separate from restoration of youthful appearance. This technique has the advantage of adjustability in very small increments to create small changes that can not be produced reliably using surgical techniques. Often, patients who are actors, models, or in similar careers need very small shape adjustments to improve symmetry or refine the details of their appearance. Substantial changes are best addressed with solid facial implants or osteotomies. Fillers also have a role in camouflaging the visible edge of an implant, especially in the very thin patient or the patient with a very large implant.
Nasolabial fold
This treatment area, which represented the test bed for most of the studies of FDA-approved fillers, remains a mainstay of clinical treatment. Although it has fallen into disfavor with some, because it is not a prominent aging feature or is better corrected with filler cheek augmentation, it is included in most of this author’s treatment planning for naïve or relatively inexperienced patients. Patients in their late 30s and early 40s or beyond almost always benefit from a modest appropriate amount of correction of the nasolabial fold.
The depth increases with aging in most patients, but other features need to be assessed during treatment planning. Asymmetries need to be assessed and demonstrated to the patient before treatment. These asymmetries will be blunted by filler augmentation, but rarely completely eliminated. The degree of depth correction needs to be modest and natural looking. The nasolabial fold is a normal facial feature in youth and should not be completely effaced or bulging with convexity at any point.
In addition to nasolabial depth, the presence of any dermal rhytid along the length of the fold should be noted. In patients with a rhytid, this author selects an HA filler that can be placed both in the deep dermis or dermal subcutaneous junction as well as in the mid dermis for more complete correction of the rhytid as well as fold depth. Alternatively, CaHa can be selected for deep correction at the dermal subcutaneous junction followed by middermal correction of the rhytid. This bilayer treatment can be done in 1 sitting or in an alternating fashion. Patients need to be questioned about which feature of the fold they find most objectionable; some patients have a strong prioritization to focus on correction of the rhytid rather than the depth or the other way around.
The final assessment is the presence or absence and severity of overhanging inferomedial cheek skin, which will also modulate the injection technique. Severe skin overhang is best corrected with facialplasty or a middle facelift to resuspend the cheek. Moderate skin redundancy here ideally requires cross-hatching transversely across the fold to better flatten and structure the skin surface conformation, as well as some filler cheek augmentation. Mild redundancy is usually amenable to cross-hatching alone. The absence of any noticeable degree of skin redundancy is ideal for a fold-only volume fill with a fanning technique. Treatment can proceed without following this protocol, but the patient should be cautioned of this compromise and the resulting incomplete correction of overhanging skin.
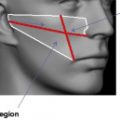
For basic fold filling, a fanning technique is used, inserting the needle inferiorly on the fold and advancing it superiorly to the apex at the base of the nose ( Fig. 1 ). Injection is made retrograde placing 0.05 to 0.1 mL of material in each pass until optimal correction is obtained. Both CaHa and HA work well in this area, preferably mixed with 0.2 to 0.3 mL of 1% lidocaine with epinephrine to help minimize ecchymosis. It is more difficult to produce an overfilled look or an unnatural surface feature with subdermal rather than intradermal placement of filler.