16 Infraorbital hollow and nasojugal fold
Summary and Key Features
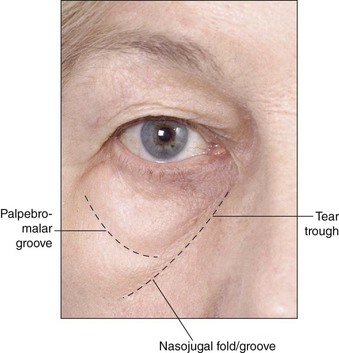
• The infraorbital hollow (IOH) refers to the U-shaped or curvilinear depression under the eyes and comprises the tear trough, nasojugal fold, and palpebromalar groove and has become a common presentation for those seeking cosmetic enhancement to the lower eyelid and mid-face
• With thin skin overlying bone and little to no subcutaneous fat or muscle in this region, the IOH can be an unforgiving region and challenging to treat with injectable agents
• Injections seem to work best in patients with thick and smooth skin and a well-defined tear trough, without excessively protruding eyelid fat or excess eyelid skin
• Hyaluronic acid is currently the injectable agent treatment of choice for IOHs and lower eyelid / periorbital augmentation
• Meticulous injection with small volumes, reduced volume speed, supraperiosteal placement, lower gauge needles and / or cannulas, and minimal number of injection sites will reduce the risk of complications
• Some patients are not suited to fillers alone and require adjuvant therapy or surgery for further restoration of the IOH
Introduction
The infraorbital hollow (IOH) refers to the curvilinear or U-shaped depression under the eyes from the nasal bone to the outer corner of the eye and comprises three core elements: the ‘tear trough’ and nasojugal fold medially, and the palpebromalar groove laterally (Fig. 16.1). Although the terms ‘tear trough’ and ‘nasojugal fold’ have historically been used interchangeably, the former – which occurs mildly in all people across all ages – refers to the superior aspect of the latter. A sign of early aging, the deepening of the tear trough leads to a true indentation at the junction of the thin eyelid skin above and thicker skin of the cheek below. Later, the mid-cheek may descend, accentuating a flat or hollow crescent below the eye. The appearance of hollows and dark circles under the eye is the interplay of various factors. Genetics and habits / environmental exposures lead to dyschromias and pigmentation; soft tissue laxity, subcutaneous volume alterations, changes in bony landmarks, and redistribution of superficial fat all lead to shadowed contours and deepening folds. Periorbital volumetric shifting and loss is not an isolated event but part of a global shift in the contours of the aging face.
There is little to no superficial fat under the lower eyelid. The orbicularis oculi muscle has direct bony attachment for approximately one-third of the orbital rim length, from the nasal bone to the medial limbus. Laterally, orbicularis-retaining ligaments connect the deep surface of the skin to bone. Retaining ligaments weaken, facial bones recede, and volume decreases in the deep fat pads, causing the cheek to descend and superficial fat to accumulate under the eye, all of which combine with genetically predisposed discolorations and bony changes to produce the perception of hollowed and sometimes baggy eyes, deep and shadowed tear troughs, and an aged, fatigued appearance refractory to cosmetic attempts at concealment (Fig. 16.1).
Candidates for augmentation of the infraorbital hollow
Proper patient selection is critical and relies on careful ophthalmologic and medical history and physical assessment. Poor candidates are unlikely to obtain optimal results and may not be satisfied with results and are at higher risk of side effects, such as visibility and irregularity (Table 16.1). Patients with diseases or metabolic conditions that predispose to lower eyelid irregularity or bleeding and infection should be excluded, and all manner of anticoagulant medications and supplements discontinued if medically safe for at least 2 weeks prior to treatment. Some patients have genetically determined pigmentation that may look like a tear trough but without an indentation that can be filled. Pigmented dark lower eyelid circles cannot be improved by fillers and can, in fact, be worsened by treatment. Older patients with thinner, crepe-like, inelastic skin and individuals with pre-existing malar edema – whether metabolic (thyroid disease) or otherwise (i.e. chronic sinus disease, prior surgery, etc.) – may not respond well and also have an increased risk for adverse events and dissatisfaction with these treatments. Patients with orbital fat herniation and significant skin laxity would benefit first from lower lid blepharoplasty or other surgical procedures. Injection works best in patients with thicker and smooth skin and a well-defined tear trough or defined maxillary retrusion / hypoplasia (common in young Asian females), without excessively protruding eyelid fat or excess eyelid skin.
Table 16.1 Identifying candidates for augmentation of the infraorbital hollow
| Best candidates | Poor candidates |
|---|---|
| Young patients with good skin elasticity | Elderly patients with poor skin elasticity |
| Thick smooth skin | Very thin skin |
| Good skin tone | Transparent or dyspigmented skin |
| Minimal laxity | Significant skin laxity |
| Mild-to-moderate tear troughs | Extremely deep tear troughs |
Appropriate filling agents
The use of autologous fat had gained popularity in recent years (also) as a replacement for surgery for the correction of contour defects and has been used for augmentation of the IOH, but results have been generally unpredictable and often associated with considerable side effects such as lumpiness, long-lasting irregularities, volume distortion, and prolonged edema, as well as risks associated with any surgical procedure. More recently, hyaluronic acid (HA) – with its gel consistency, varying concentrations and the possibility of dilution with lidocaine or saline, favorable flow characteristics, fewer side effects, and non-permanence – has emerged as the treatment of choice for augmentation of the lower periorbita by injection. Lumps or irregularities can be avoided with careful and precise injection techniques and can also be reversed through treatment with hyaluronidase, an important consideration when injecting in delicate areas requiring precise placement of filling agent. Surprisingly, HA in the periorbital region yields better than expected longevity. Lambros (and others) have described the persistence of effect, often in excess of 1 year (see Ch. 15). Donath and colleagues used three-dimensional imaging in 20 patients treated in the tear trough with HA and found an average 85% maintenance of effect at the final follow-up visit (average 14.4 months); the patient with the longest duration retained 73% volume augmentation at 23 months without any touch-ups. Side effects with HA can include visibility and nodules, a bluish tint (from the presumed Tyndall effect), along with injection-related bruising and swelling (see Complications).





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


