CHAPTER 18 Inferior Pedicle Breast Reduction Using a Circumvertical Pattern

Introduction
For many years, the preferred method for performing breast reduction has combined the use of an inferiorly based pedicle with an inverted T or ‘Wise’ skin pattern and many reports have documented the success of this technique in reducing the symptomatically enlarged breast.1–6 However, it is possible to combine the inferior pedicle approach with a short scar circumvertical skin pattern to accomplish the same reduction in volume with a much less significant scar burden. This procedure, called the short scar periareolar inferior pedicle reduction or SPAIR mammaplasty7–9 is applicable to breasts of all sizes and provides aesthetic, long-lasting results in a consistent fashion. This chapter will outline the markings, operative technique, and results of this versatile method of breast reduction.
Patient Selection
While pedicle length is an important variable that can influence the subsequent development of ischemia to the NAC, another anatomic feature of the breast that directly affects the vascularization of the inferior pedicle relates to the identification and preservation of the internal breast septum.10–12 This septum, which has a cranial and caudal leaf, runs transversely within the breast at the junction of the lower third with the upper two-thirds and most likely represents a traction imbrication as the enlarging breast folds over itself as it hypertrophies (Fig. 18.1). Within this septum run several sizable intercostal perforators that provide direct axial blood flow to the inferior pedicle. As such, the septum functions as a neurovascular mesentery. The septum is easily identified in most patients during skeletonization of the inferior pedicle (Fig. 18.2). Once the redundant tissue is removed from the apex of the pedicle near the base of the breast, the mesenteric space can be seen to present a mobile interface as the cranial and caudal layers slide past one another. Preserving this vascular mesentery becomes a critical technical maneuver when attempting to ensure adequate vascularization of the inferior pedicle.
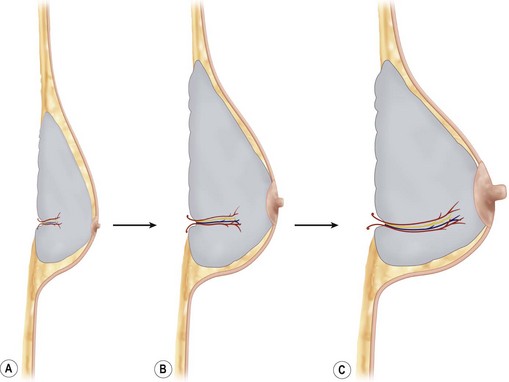


With permission from Hammond DC. Atlas of aesthetic breast surgery. Elsevier; 2008, Figs 16.1–16.8C.
Operative Technique
Marking
When marking the patient for an inferior pedicle circumvertical procedure, the basic goal is to determine that portion of the redundant skin envelope that will need to be preserved so as to easily wrap around the inferior pedicle in a contoured fashion to create the most aesthetic result. To accomplish this task, four cardinal points are identified that will define that portion of the skin envelope that will be preserved. Initially, basic orientation marks are applied to identify the inframammary fold on each side, the midsternal line and the breast meridian (Fig. 18.3A–D). It should be noted that the breast meridian does not necessarily run through the nipple as often the NAC is malpositioned either medially or laterally. As well, it is a very useful maneuver to draw a line across the midline connecting the two inframammary folds. This allows the location of the fold to be visualized without manipulating and possibly distorting the position of the breast. The first cardinal mark is located by drawing a line that parallels the inframammary fold line 4 cm above the inframammary fold. Where this line intersects the breast meridian on each side represents the top of the periareolar pattern (Fig. 18.3E). The inferior cardinal point is identified by drawing an 8 cm wide pedicle that extends up to the NAC centered on the breast meridian (Fig. 18.3F






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


