Inferior Gluteal Artery Perforator Flap Breast Reconstruction
Katie E. Weichman
DEFINITION
Fujino et al. first popularized the gluteal donor site for breast reconstruction in 1975 as a free myocutaneous flap, and Shaw further refined it in 1983.1,2 Additional modification of this myocutaneous flap by Paletta and Le-Quang et al. to use the inferior gluteal vessels as donor vessels was also described. However, despite initial success, it was abandoned secondary to technical difficulty and postoperative morbidity to the sciatic nerve.
After the popularization of perforator flaps by Koshima, both the inferior and superior gluteal artery perforator flaps were described and gained popularity in reconstructive surgery.
The inferior gluteal artery perforator (IGAP) flap was first described as a pedicled flap for ischial pressure sores by Blondeel in 2002.
Allen further expanded the IGAP flap for breast reconstruction in 2004.3 He further advanced this perforator flap, with a widely accepted in-crease technique. This technique uses skin and tissue in the buttock area based on the IGAPs and minimizes the scar in the gluteal crease.4
Though abdominally based free flaps remain the most common choice for breast reconstruction secondary to sufficient skin and soft tissue, patients may require alternative donor sites for various reasons. These reasons include lack of abdominal donor sites secondary to prior abdominoplasty, inadequate volume in the abdomen, and patient preference. Approximately 20% of patients are not candidate for abdominally based free flaps.2
Advantages of IGAP flaps include the ability to harvest as a sensate flap (posterior cutaneous nerve of the thigh), hidden donor site, lack of risk of abdominal hernia/bulge, and increased breast projection based on the consistency of the buttock fat. Additionally, IGAP has a slightly longer pedicle when compared to SGAP, and the risks of aesthetic donorsite morbidity with increased beveling of adjacent fat are decreased.
Disadvantages include difficult patient positioning in bilateral cases, tedious dissection with a long oblique intramuscular course, potential injury to sciatic or posterior femoral cutaneous nerves, and significant arterial and venous mismatch of the pedicle.
ANATOMY
The inferior gluteal artery originates from the internal iliac artery and is the smaller of its terminal branches. It exits the pelvis through the greater sciatic foramen and accompanies the greater sciatic nerve, internal pudendal artery and vein, and the posterior femoral cutaneous nerve.
Anatomically, after perforating the sacral fascia, the inferior gluteal vessels exit below (caudal) to the piriformis muscle and above (cranial) to the coccyx (FIG 1).
Once it exists below the piriformis, it divides into several perforators, usually more than the SGAP flap, and then travels in an intramuscular fashion to supply the inferior portion of the buttock.
The length of the perforator depends on the area of the buttock supplied. Inferomedial perforators tend to be shorter with less intramuscular course (3-5 cm), whereas superolateral perforators tend to have a longer intramuscular course (4-6 cm). Therefore, lateral perforators are preferentially chosen for longer pedicle length.
In 91% of patients, the inferior gluteal vessels travel with the posterior femoral cutaneous nerve (S1-S2) to the posterior thigh.5 Therefore, if desired, a neurosensory flap is possible if nerves are preserved.
The inferior gluteal vein is associated with the inferior gluteal artery; however, it receives multiple tributaries in the subsacral fascia fibroconnective tissue. These vessels are prone to bleeding at the level of the pelvis and are quite large and friable. These vessels are routinely larger than superior gluteal veins.
The perforating vessels, which are all musculocutaneous, are located inferior to the exit point below the piriformis muscle.
Several studies have looked at these perforating vessels and found IGAP flaps have a mean number of 7 perforators (range 4-10), with an average intramuscular length of 8.7 cm (range 6-14 cm) and a mean total pedicle length of 13.4 cm (range 10-17 cm). Additionally, the mean main vessel diameter was found to be 5 mm (range 4-7 mm) for the inferior gluteal artery and 7.7 mm (range 6-10 mm) for the inferior gluteal vein.6
Understanding the course of the sciatic nerve and the posterior femoral cutaneous nerve is paramount to this flap
dissection. These nerves often run together with the inferior gluteal artery as it emerges from the sciatic foramen below the piriformis muscle. The posterior cutaneous nerve is generally more medial in relation to both the inferior gluteal artery and sciatic nerve. Both nerves run posterior to the gluteus maximus muscle.
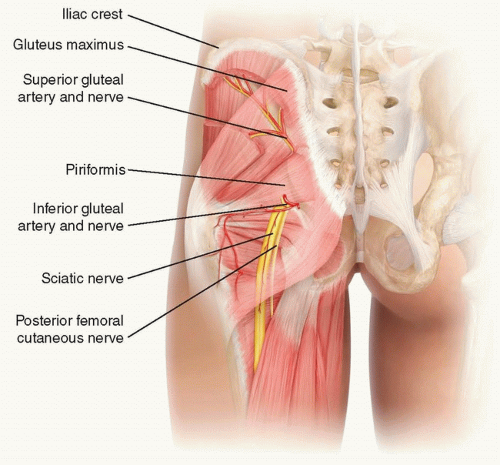
FIG 1 • Location of the inferior gluteal artery in relation to the piriformis muscle, posterior femoral cutaneous nerve, and sciatic nerve as it penetrates the sacral fascia, the space behind the gluteus maximus muscle.
Sciatic nerve
The nerve is generally visualized during the submuscular dissection below the sacral fascia, as it exits the sciatic foramen below the piriformis muscle and travels posterior to the gluteus maximus muscle and anterior to the inferior gemellus muscle.
Provides motor and sensory control to almost the entire posterior leg and foot
Derived from spinal nerves L4-S3 and is the largest, widest, single nerve in the body
Posterior femoral cutaneous nerve (S1-S2)
Can be observed at two points during the dissection
First, along the inferior incision of the skin paddle, in the gluteal crease, in the subfascial plane, where the investing muscular fascia of the gluteus maximus muscle and fascia lata coalesce
Second, during submusclar/subfascial dissection proximally with the inferior gluteal artery pedicle and sciatic nerve
Provides sensation to the posterior thigh, leg, and perineum
Derived from the sacral plexus and has three main branches:
Inferior cluneal nerves (most likely encountered on inferior skin paddle incision)
Three of four in number
Turn upward around the lower border of the gluteus maximus
Provide sensibility to the skin covering the lower lateral portion of the gluteus maximus
Perineal branches
Supply the skin covering the perineum
Main continuation in the posterior thigh
Travels posterior to fascia lata anterior to long head of biceps femoris
In mid leg, pierces fascia and travels with the lesser saphenous vein in the subcutaneous plane
Provides sensation to posterior and medial thigh, popliteal fossa, and superior leg
There are several muscles that are highlighted for IGAP dissection in the posterior gluteal area.
Gluteus maximus
Origin: Gluteal surface of the ilium, lumbar fascia, sacrum, and sacrotuberous ligament
Insertion: Gluteal tuberosity of the femur and iliotibial tract
Action: External rotation and extension of the hip joint
Arterial supply: Superior and inferior gluteal arteries
Innervation: Inferior gluteal nerve (L5, S1, and S2)
Gluteus medius (deep to the gluteus maximus)
Origin: Gluteal surface of the ilium
Insertion: Greater trochanter of the femur forming the iliotibial tract
Action: Abduction of the hip, preventing adduction of the hip, and medial rotation of the thigh
Piriformis (deep to the gluteus maximus)
Origin: Anterior portion of the sacrum
Insertion: Greater trochanter of the femur forming the iliotibial tract
Action: External rotator of the thigh
Arterial supply: Interior gluteal artery, superior gluteal artery, and lateral sacral artery
Innervation: Nerve to the piriformis (L5, S1, and S2)
Gluteus minimus (deep to gluteus maximus and gluteus medius)
Origin: ilium under the gluteus minimus
Insertion: greater trochanter of the femur forming the iliotibial tract
Action—works in concert with gluteus medius: abduction of the hip, preventing adduction of the hip, and medial rotation of the thigh
Arterial supply: superior gluteal artery
Innervation: superior gluteal nerve (L4, L5, S1)
PATIENT HISTORY AND PHYSICAL FINDINGS
This includes patients with a history of breast cancer, patients undergoing prophylactic mastectomy, patients with congenital abnormalities, and transgender patients.
Physical examination includes examination of the abdomen, medial thighs, and buttock to assess availability of excess tissue.
Patients who are candidates for IGAP flap are generally nulliparous, with inadequate abdominal soft tissue, prior abdominoplasty, prior abdominal flap harvest, or prior abdominal liposuction.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








