In the plastic surgery patient population, outpatient surgery is cost effective and will continue to grow as the preferred arena for performing surgery in healthy patients. Although there is a widespread myth that outpatient surgery centers may suffer from increased infection rates due to lax infection control, the data presented from American Association for Accreditation of Ambulatory Surgery Facilities–accredited facilities prove the contrary. There is a lack of data investigating infection prevention in the perioperative period in plastic surgery patients. As data collection becomes more refined, tracking the postoperative care environment should offer additional opportunities to lower the incidence of postoperative infections.
Key points
- •
In the plastic surgery patient population, outpatient surgery is cost effective and will continue to grow as the preferred arena for performing surgery in healthy patients.
- •
Although there is a widespread myth that outpatient surgery centers may suffer from increased infection rates due to lax infection control, the data presented from American Association for Accreditation of Ambulatory Surgery Facilities (AAAASF)–accredited facilities prove the contrary.
- •
There is a lack of data investigating infection prevention in the perioperative period in plastic surgery patients.
- •
As data collection becomes more refined, tracking the postoperative care environment should offer additional opportunities to lower the incidence of postoperative infections.
Introduction
Over the last decade, surgical care in the United States has shifted to an ambulatory surgical setting, where enormous growth has been seen. Ambulatory surgical centers are defined by the Centers for Medicare & Medicaid Services as facilities that operate exclusively to provide surgical services to patients who do not require hospitalization or stays in a surgical facility longer than 24 hours. Between 2001 and 2008, there was a greater than 50% increase in the number of Medicare-certified ambulatory surgical centers in the United States. In 2007, these facilities performed more than 6 million procedures. According to Reuters, as of 2011, more than 57 million outpatient surgeries took place in the United States in more than 5000 surgery centers nationwide. With efforts to boost cost-savings, three-quarters of surgeries are done on an outpatient basis.
With growth in this sector, there have been articles written that express concern about the level of infection control in the outpatient surgery environment. These concerns have been fueled by some high-profile examples of lapses in prevention. Between 1998 and 2008, 448 people acquired hepatitis B or hepatitis C infection linked to outpatient care in 33 outbreaks. In a 2010 JAMA article, an audit of 68 centers in 3 states participating in a pilot inspection program found that approximately two-thirds (67.6%) had a lapse in at least 1 of 5 infection control categories. Although only a pilot study, these findings set off concerns about potentially serious lapses in infection control in several states.
The Centers for Disease Control and Prevention assess 5 categories of infection control: hand hygiene and personal protective equipment, injection safety and medication handling, equipment reprocessing (eg, sterilization and high-level disinfection), environmental cleaning, and handling of blood glucose monitoring equipment. The Centers for Disease Control and Prevention have found errors in basic infection control practices in the outpatient setting and, as a result, the reputation of outpatient surgery centers has suffered. More recent findings, however, in an extensive review of the data collection from the AAAASF, suggest that outpatient surgeries performed in accredited centers have low infection rates.
Introduction
Over the last decade, surgical care in the United States has shifted to an ambulatory surgical setting, where enormous growth has been seen. Ambulatory surgical centers are defined by the Centers for Medicare & Medicaid Services as facilities that operate exclusively to provide surgical services to patients who do not require hospitalization or stays in a surgical facility longer than 24 hours. Between 2001 and 2008, there was a greater than 50% increase in the number of Medicare-certified ambulatory surgical centers in the United States. In 2007, these facilities performed more than 6 million procedures. According to Reuters, as of 2011, more than 57 million outpatient surgeries took place in the United States in more than 5000 surgery centers nationwide. With efforts to boost cost-savings, three-quarters of surgeries are done on an outpatient basis.
With growth in this sector, there have been articles written that express concern about the level of infection control in the outpatient surgery environment. These concerns have been fueled by some high-profile examples of lapses in prevention. Between 1998 and 2008, 448 people acquired hepatitis B or hepatitis C infection linked to outpatient care in 33 outbreaks. In a 2010 JAMA article, an audit of 68 centers in 3 states participating in a pilot inspection program found that approximately two-thirds (67.6%) had a lapse in at least 1 of 5 infection control categories. Although only a pilot study, these findings set off concerns about potentially serious lapses in infection control in several states.
The Centers for Disease Control and Prevention assess 5 categories of infection control: hand hygiene and personal protective equipment, injection safety and medication handling, equipment reprocessing (eg, sterilization and high-level disinfection), environmental cleaning, and handling of blood glucose monitoring equipment. The Centers for Disease Control and Prevention have found errors in basic infection control practices in the outpatient setting and, as a result, the reputation of outpatient surgery centers has suffered. More recent findings, however, in an extensive review of the data collection from the AAAASF, suggest that outpatient surgeries performed in accredited centers have low infection rates.
Data on infection rates in outpatient surgery from AAAASF
Data collected from AAAASF-certified surgery centers from 2001 to 2012 ( Table 1 ) analyzed outcomes from 5,416,071 operations, where 7,629,686 procedures were performed (1.41 procedures per case). Plastic surgery cases comprised 3,922,202 of these operations and 5,525,255 of the procedures (also, 1.41 procedures per case).
| Total cases all AAAASF specialties | 5,416,071 | ||
| Total procedures all AAAASF specialties | 7,629,686 | 1.41 | Procedures per case |
| Plastic surgery cases | 3,922,202 | ||
| Plastic surgery procedures | 5,525,255 | 1.41 | Procedures per case |
The total number of untoward operative sequelae from these 3,922,202 plastic surgery cases was 21,944 (0.4052%); that is, 1 in 247 plastic surgery cases or 1 in 348 plastic surgery procedures had a complication ( Table 2 ). Of these complications, 3063 were infections (0.0781%). Infections developed in 1 in 1281 plastic surgery cases and 1 in 1804 plastic surgery procedures. The infection rate as a percentage of all untoward sequelae was 13.96%.
| Incidence Percentage by Case | 1 in # Case | Incidence Percentage by Procedure | 1 in # Procedure | ||
|---|---|---|---|---|---|
| Total plastic surgery sequelae | 21,944 | 0.41% | 247 | 0.29% | 348 |
| Total plastic surgery infections | 3063 | 0.08% | 1281 | 0.06% | 1804 |
| Infections as percentage of sequelae | 13.96% |
a Incidence of infection by case and procedure. Infection as a percentage of all plastic surgery sequelae.
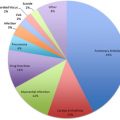
In this data set, infection was most commonly reported, in order from highest to lowest, in the following procedures: breast augmentation, abdominoplasty, breast lift/reduction, liposuction, and facelift ( Table 3 ). Although more infections were reported with breast augmentation surgery, there were more breast augmentations performed and the rate of infection was lower than in patients undergoing abdominoplasty. Therefore, the rate of infection per procedure, from highest to lowest, was as follows: abdominoplasty, breast lift/reduction, breast augmentation, liposuction, and facelift.
| Procedure | Number of Infections | Number of Cases | Rate of Infection (%) | 1 in |
|---|---|---|---|---|
| Breast augmentation | 921 | 1,125,274 | 0.08 | 1222 |
| Abdominoplasty | 757 | 462,588 | 0.16 | 611 |
| Breast lift/reduction | 582 | 515,252 | 0.11 | 885 |
| Liposuction | 517 | 688,241 | 0.08 | 1331 |
| Facelift and related procedures | 346 | 499,477 | 0.07 | 1444 |
A total 462,588 abdominoplasties were performed and 757 cases of infection reported. This is a 0.16% infection rate (1 in 611 patients) from abdominoplasty. Also, 1,125,274 breast augmentation procedures were evaluated and 921 infections reported, resulting in a 0.08% incidence of infection or 1 in 1222 patients; 515,252 patients underwent breast lift/reduction with 582 reported infections, which is a 0.11% infection rate, or 1 in 885 breast lift/reduction patients; 517 of 688,241 liposuction patients had reported infection—0.08% or 1 in 1331 liposuction patients; and 346 of 499,477 facelift patients developed infection—0.07% or 1 in 1444 facelift patients (see Table 3 ). The most commonly cultured organism was Staphylococcus ( Table 4 ). No organisms were found or no culture was taken in 420 cases. Methicillin-resistant Staphylococcus aureus (MRSA) was cultured in 86 cases.
| Organism | Number of Cases |
|---|---|
| Staphylococcus | 376 |
| Culture not done | 240 |
| No growth | 180 |
| MRSA | 86 |
A total 225 plastic surgery patients had to be hospitalized due to postoperative infection. Most commonly, these patients requiring hospitalization had undergone, in order of most common to least common: abdominoplasty, breast augmentation, liposuction, breast lift/reduction, and facelift ( Table 5 ). The specific incidences of infection requiring hospitalization from each plastic surgery procedure are as follows: 1 in 5782 abdominoplasty patients; 1 in 32,151 breast augmentation patients; 1 in 36,804 breast lift/reduction patients; 1 in 45,883 liposuction patients; and 1 in 49,948 facelift patients (see Table 5 ). The most commonly found organism in these patients was also Staphylococcus ( Table 6 ). Cultures were not performed in 20 cases and cultures were negative in 12. MRSA was present in 9 patients requiring hospitalization because of infection.
| Procedure | Number of Hospitalizations | Number of Cases | Rate of Infection | 1 in |
|---|---|---|---|---|
| Abdominoplasty | 80 | 462,588 | 0.0173% | 5782 |
| Breast augmentation | 35 | 1,125,274 | 0.0031% | 32,151 |
| Liposuction | 15 | 688,241 | 0.0022% | 45,883 |
| Breast lift/reduction | 14 | 515,252 | 0.0027% | 36,804 |
| Facelift and related procedures | 10 | 499,477 | 0.0020% | 49,948 |
| Total | 225 |
Related posts:
 Conscious Sedation/Local Anesthesia in the Office-Based Surgical and Procedural Facility
Conscious Sedation/Local Anesthesia in the Office-Based Surgical and Procedural Facility
 Deep Vein Thrombosis Chemoprophylaxis in Plastic Surgery
Deep Vein Thrombosis Chemoprophylaxis in Plastic Surgery
 Airway Management in the Outpatient Setting
Airway Management in the Outpatient Setting
 Outpatient Surgery and Sequelae
Outpatient Surgery and Sequelae
 Management of Postoperative Nausea and Vomiting in Ambulatory Surgery
Preventing Surgical Mishaps
Management of Postoperative Nausea and Vomiting in Ambulatory Surgery
Preventing Surgical Mishaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


