CHAPTER 9 Indications for Primary Total Hip Arthroplasty
INDICATIONS
The diagnostic indications for THA most commonly include primary osteoarthritis, inflammatory arthritis, avascular necrosis, femoral neck fracture, femoral neck nonunion or malunion, and hip dysplasia. The indications for THA from over 8100 THAs performed at our institution over the past 20 years are represented in Table 9-1. Each indication is discussed in detail in this chapter. Osteoarthritis was the most common indication for THA, followed by avascular necrosis, inflammatory arthropathies, and following proximal femoral fracture.
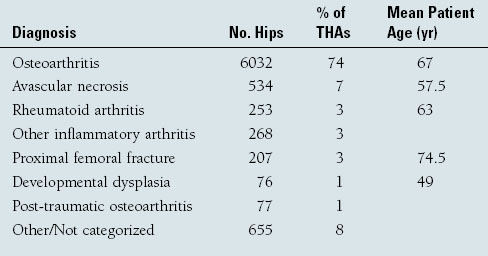
Patient age is a factor to consider in the context of considering the indications for THA. Younger individuals may greatly benefit from the pain relief and functional improvement from a THA but need to be informed that they are at risk for single or multiple revisions in their lifetime. “Waiting as long as possible” is often a wise concept, but many patients with advanced avascular necrosis, developmental dysplasia of the hip, or rheumatoid arthritis still make excellent candidates due to their high levels of pain and functional impairment. These diagnoses are found in younger patients undergoing THA in our series (see Table 9-1). The surgeon should consider appropriate implant fixation interfaces and bearing surfaces in patients in whom the implant may be required to last into a third decade of use, as is the case with many younger individuals.1–4
Primary osteoarthritis of the hip is the most common indication for THA at our center (see Table 9-1) and in most series of THA (Fig. 9-1). Osteoarthritis may result from many causes and has been demonstrated to affect the medial, superior, and lateral aspects of the hip.5 The location of osteoarthritis has implications on implant selection and survivorship. Mechanical cam-type impingement from malalignment, slipped capital femoral epiphysis, or Legg-Calvé-Perthes disease has been associated with hip arthrosis, most notably in younger individuals. Cam impingement has recently become the focus of nonarthroplastic treatment of early hip disease through osteotomy and débridement techniques6 and has been discussed in preceding chapters.

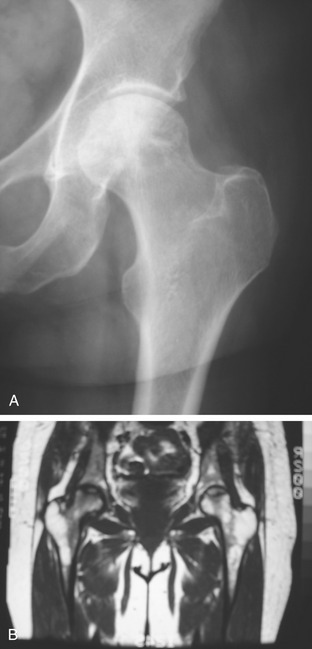
Avascular Necrosis
Avascular necrosis results in loss of femoral head integrity and eventual collapse of subchondral bone with resulting joint incongruity (Fig. 9-2A). MRI helps confirm the diagnosis when plain radiographs are inconclusive (see Fig. 9-2B). Causes of avascular necrosis include excess alcohol consumption, systemic corticosteroid administration, displaced femoral neck fractures, traumatic hip dislocations, irradiation, or idiopathic categories.7 Osteonecrosis following irradiation of the pelvis is an indication for THA. Implant selection is important because both cemented and uncemented implants have been reported to have decreased clinical survivorship in hips that have been irradiated,8 although in recent years total hip arthroplasty using modern generation uncemented components in patients with irradiated pelvis has had encouraging outcomes.9