div class=”ChapterContextInformation”>
5. Adherence in Pediatric Populations
Keywords
AdherenceCompliancePediatric populationsAdolescentsParentsCaregiversFamily dynamicsWritten action plansEducational interventionsDermatologyAtopic dermatitisIntroduction
Upwards of 50% of pediatric patients with chronic health conditions are considered to be nonadherent to medical treatment regimens. As such, improving self-management and adherence are paramount to not only improving health outcomes, but pediatric adjustment to chronic disease. Dermatologic conditions in pediatric populations put children at an increased risk for low self-esteem, depression, anxiety, social isolation, and suicidal ideation [1]. Social reactions to cutaneous disease are more devastating to pediatric populations, and appearance-related concerns are one of the dominant experiences of adolescents [2]. The impact of skin conditions on a pediatric patients’ quality of life warrant early recognition and treatment to decrease their risk of physical and psychologic morbidity.
Treatment adherence is particularly challenging in pediatric populations because of family dynamics and functioning, caregiver and child characteristics, and child health outcomes. When patients are young, caregivers are often responsible for medication administration, but this responsibility shifts to the patients as they mature. This shift can complicate treatment adherence. Furthermore, both caregivers and providers should emphasize the importance of adherence in young patients to instill a sense of self-management that can persist into adulthood. Poor adherence results in poor health outcomes, which can lead to misconceptions about treatment efficacy, sometimes creating what appears to be “treatment-resistant” disease.
Promoting acceptable levels of adherence requires examining parent and child variables that facilitate or impede adherence to treatment recommendations. This chapter aims to explore the complexity of adherence in pediatric dermatology patients. We discuss barriers to adherence for the pediatric population followed by approaches that can be used to address adherence issues.
Common Barriers to Adherence in Pediatric Populations
Barriers to treatment adherence in pediatric patients/caregivers
Treatment factors |
Complicated treatment regimen |
Poor tolerability of treatment (e.g. treatment too messy, greasy) |
Time-consuming treatment regimen |
Medication cost |
Common factors between caregiver and patient |
Delayed treatment outcomes |
Mental health disorders/behavioral issues |
Caregiver/parent factors |
Poor communication |
Fear of medication side effects (corticosteroid phobia) |
Patient factors |
Age-related and developmental stage-related limitations |
Difficulty with transfer of treatment responsibility during adolescence |
Studies have demonstrated that parents with greater resources exhibit better adherence than parents with fewer resources [6]. Pediatric patients also rely on their caregiver to purchase the medication. When caregivers of pediatric dermatology patients were surveyed about factors leading to nonadherence, cost of medicine was among the most important reasons [7]. Strategies to lower medication cost include creating more cost effective treatment plans, and using generic medications when possible.
Caregiver and patient expectations set the course for treatment. For example, treatment outcomes for dermatological conditions typically occur gradually. If caregivers and patients are uninformed about the likelihood of gradual outcomes and expect full and early clearance, they may become frustrated and less adherent. Caregivers and patients also may not believe the condition as chronic, thereby requiring continuous therapy. For example, caregivers and patients may have little understanding of the maintenance role of emollients in preventing atopic dermatitis flare-ups.
Additionally, behavioral issues of patients and caregivers can undermine adherence and treatment outcomes. Children with chronic health problems are at increased risk of behavioral and emotional difficulties [8, 9]. Mood disorders, such as depression, may interfere with patient adherence because of poor concentration, fatigue, loss of interest in activities, sleep/ appetite disruption, and irritable mood [10]. Similarly, caregiver depression can hinder parental engagement in following the regimen [11]. Child behavior problems are associated with greater parent-reported difficulties with illness management [12]. Caregivers may also feel the time spent applying treatments on one child impacts the time and energy to expend on siblings and partners. If a child is resistant to receiving treatment, caregivers often pay the cost with their own emotional well-being [13].
Caregiver-Centered Barriers
Pediatric patients often rely on their parent or guardian to promote treatment adherence through the purchase and/or actual administration of medications. About 47.8% of prescriptions for children attending a dermatology outpatient clinic remained unfilled [14]. Even when medications were directly supplied to parents and regular follow-ups were provided, adherence rates were as low as 32% [15]. Pediatric patients also depend on a parent or guardian to be in attendance to consent for procedures and assist with transportation. Scheduling conflicts between caregiver and child can interfere with adherence to treatments that require frequent visits, such as phototherapy.
Caregiver concern about side effects is also a major factor in nonadherence [7]. The fear of adverse effects of topical corticosteroids is called “steroid phobia” [16]. Steroid phobia is increasingly recognized as playing a key role in poor treatment adherence, which leads to poor treatment outcomes and disease flares. Originally used to describe an irrational fear of corticosteroids, steroid phobia has been broadened to include the vague negative feelings and beliefs about using topical corticosteroids [17]. As many as 80.7% of patients reported having fears about topical corticosteroids, and 36% admitted to treatment nonadherence due to concern about steroid-related adverse effects [16]. Steroid phobia correlates with several factors, including the belief that topical corticosteroid agents pass through the skin into the bloodstream, a lack of trust in the health care provider, and discrepancies in the education about their use. Common concerns about topical corticosteroids include skin thinning, the potential of topical corticosteroids to affect growth and development, and nonspecific long-term effects. This fear can further complicate treatment as patients often initially depend on their caregivers to administer medications.
Child-Centered Barriers
Barriers to adherence that are unique to children include instructional compliance and developmental level. Children may not be aware that they have a problem, or they may not be motivated to work on it. For example, the management of atopic dermatitis is a complex process with multiple steps that have to be followed by the child. These include disrupting current activity, undressing, bathing, and receiving topical applications that may feel uncomfortable. Children are not naturally motivated to follow such complex instructions and may therefore resist implementing a treatment routine. Maintaining a treatment regimen requires the child to be under good instructional control or the child will often not comply with the program.
Developmental level also influences treatment adherence, especially when treatments require the child to actively participate. Caregivers are often responsible for medication adherence in young children, whereas adherence for older children or adolescents becomes a process of shared responsibility. Adolescence is a critical period for many children with a chronic medical condition. Adolescents often fare worse with regimen adherence than younger children across multiple pediatric conditions [18–20]. With adolescence also comes increasing general responsibility, and many caregivers and providers transition treatment responsibility to the adolescent. This transition can lead to an increase in caregiver–child conflict over treatment management and adherence [21]. Specifically, as children move into adolescence, they begin taking control of their bodies and may want more responsibility in decision making. Despite this desire for more responsibility, adolescents may need more support from caregivers and medical providers in developing and following their treatment regimens.
Adherence Assessment
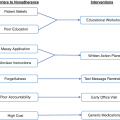
Adherence assessment
Time constraints |
Identify priorities and enhance time management |
Financial resources |
Prescribe generic, affordable options |
Work with pharmacy or insurance company on financial assistance |
Forgetfulness |
Set reminds (alarms, texts), frequent follow-up |
Regimen complexity |
Simplify regimen with combination treatments |
Prior treatments |
Discuss problems with prior treatment options and regimens |
Mental health/family issues |
Acknowledge, assess, normalize, and validate |
Involve psychologist if necessary |
During these discussions, providers should also screen for psychosocial factors and stress associated with pediatric dermatologic disorders, including the important role of mental health. Challenges facing caregivers of children with chronic health conditions include competently and consistently implementing a treatment regimen to which the child may be uncooperative or resistant [22]. Addressing mental health issues or problematic family functioning and communication may be necessary for optimizing adherence. Families can also be referred for psychological care when family communication strategies limit the ability to effectively share treatment responsibilities, especially among adolescents, or when parental mental health issues (eg, depression) impede treatment management.
If the patient and caregivers feel that their concerns to the successful implementation of the medical regimen have not been addressed, then they will likely be less successful in adhering [23]. Medical providers should ensure that caregivers and patient understand the logistics of completing their medical regimen and that following the medical regimen will lead to improved health outcomes.
Approaches and Techniques to Facilitate Treatment Adherence
Setting the stage for enhancing treatment adherence with children and adolescents generally involves attending three broad areas: (a) relationship building and support, (b) education, and (c) skills training and motivation. Meta-analyses of treatment adherence suggested that when interventions use more than one strategy for improving adherence, they are more effective [24–26].
Relationship Building and Support
Relationship building and support
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


