The management of mutilated upper extremity wounds offers challenges for all hand surgeons. Loss of composite tissues usually requires grafts or flaps to gain coverage and restore function. Nonsalvagable digits or amputated parts are a source of spare tissues that can be used for reconstruction of the hand or limb. Immediate tissue transplantation is a resourceful technique for hand surgeons to limit donor morbidity while making the most out of a terrible injury to the hand or upper extremity. This article reviews the various methods by which immediate tissue transplantation can be employed in hand trauma.
Key points
- •
All tissues of a traumatized digit, hand, or upper extremity should be evaluated for the possibility for the use of immediate tissue transplantation.
- •
The initial principles in treating a mangled extremity should always apply.
- •
Early debridement and irrigation followed by bony stabilization, tissue repair, reconstruction, and soft tissue coverage are crucial to a successful limb salvage.
- •
These are the tissues that can be utilized in immediate tissue transplantation.
- •
Although attempts are made to minimize donor site morbidity, there are times when this donor morbidity may be significant.
- •
The use of spare parts minimizes donor site morbidity while preserving as much function as possible.
The concept of spare parts surgery is not new to surgeons who treat patients with mutilating hand trauma. In 1947, Cave described using skin from dysfunctional digits to cover hypothenar wounds sustained through a gunshot wound. Some hand or upper extremity injuries do not lend themselves to the possibility of simple repair of tissues, joints, or bones. Loss of tissues in trauma often requires the harvesting of distant tissues for reconstructive purposes. Vein grafts, nerve grafts, tendon grafts, bone grafts, and soft tissue coverage are integral in the reconstructive surgeon’s armamentarium.
Each graft used for reconstructive purposes, however, would necessarily require the utility of some type of donor site unless pieces of tissue that might normally be discarded can be exploited to act as the grafts needed in the reconstruction. Immediate tissue transplantation, also known as spare part surgery, employs the principles that mangled hands or upper extremities may not be able to be replanted or repaired anatomically but may have some undamaged tissues that can be moved from their original body part to serve another area that requires reconstruction.
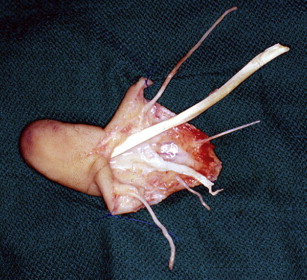
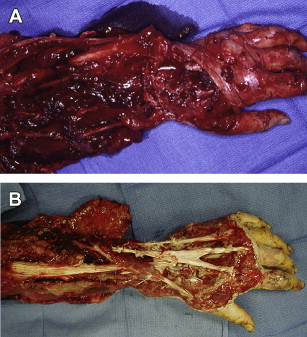
Many opportunities to use the spare parts surgery arise from amputated hands or arms. Over 100,000 digital amputations occur each year in the United States. Fewer than 30% are replanted. Nonreplantable amputated parts may provide tissue pieces that can be used as grafts. The patient, then, is not subjected to further mobility in other parts of their body by harvesting tissues for grafts or flaps. For the most part, any tissue that is somewhat preserved can be used as spare parts. A table saw injury that renders 1 digit not replantable, may supply the others injured digits with nerve grafts, nailbeds, skin grafts, tendon grafts, bone grafts, or even vascularized joints, bone, or filleted fasciocutaneous flaps ( Figs. 1 and 2 ). Arm amputations that have surpassed the allowable ischemia time may provide vascularized forearm fasciocutaneous fillet tissue to cover residual exposed bones. Spare part tissue transplantation can also be used for more than 1 function. Reports of immediate tissue transplantation for soft tissue coverage and restoration of circulation using the flap as a flow-through conduit have demonstrated this technique.
The guiding principles of immediate tissue transplantation surgery for the upper extremity are included in Box 1 . There are many types of immediate tissue transplantation. Box 2 illustrates the various methods by which tissue can be mobilized, transferred, or utilized in spare part reconstruction. Grafts are rather self-explanatory, in that, any tissue needed is dissected from its parent part to fill a void in the injured hand or upper extremity ( Fig. 3 ). The fillet flaps are used for soft tissue coverage of the hand or other areas of the extremity. The fillet flaps or transplants are transferred as a pedicled flap with the vascularity remaining intact, or as a free flap. Digits are filleted by making a midline incision on their volar aspect, removing the bone and tendons. The flap survives on the digital arteries, while the dorsal intact veins provide venous drainage. The flap can be used to cover exposed vital structures when the digit itself has been rendered not worthy of salvage ( Figs. 4 and 5 ). Fillet flaps harvested as free tissue transfers are extremely versatile, because there is no restriction of limits of transfer ( Figs. 6 and 7 ). Essentially the flap is harvested on a dominant blood vessel like the radial artery, dissected as a fasciocutaneous flap, and transferred to cover areas of exposed bone or vital structures ( Fig. 8 ). This procedure is usually performed to salvage length of a limb so that the ulna and radius can be covered without the need of performing an above-elbow revision amputation ( Fig. 9 ). By preserving elbow function, a much more functional below-elbow prosthesis can be used instead of the above-elbow prosthesis.
- 1.
Donor sites are required to perform some portion of the reconstruction of the impaired limb.
- 2.
Some portion of the amputated or mangled tissue is available for reconstruction.
- 3.
The use of available tissue will ameliorate or limit donor site morbidity.
- 4.
The lady flaps can provide coverage of exposed bone or vital structures to maintain length of a stump to improve prosthesis use.
- 5.
Replants should be performed unless contraindicated by ischemia time, level of injury, mechanism, degree of contamination, or patient stability.
- 6.
Digits rendered so badly damaged that function will never return should be considered for spare parts to other salvageable digits or areas in the upper extremity.
- 7.
Prolonged spare parts surgery should not be performed if the patient’s general condition will be or is compromised.
- 8.
Highly contaminated tissue should not be used as spare parts as this could put the patient at risk.
- 9.
Spare parts surgery can be performed as a delayed procedure if the tissue is still vascularized yet detrimental to the current function of the hand.
- 10.
Never discard any tissue until the procedure is over.
|
|
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


