Mammography showing craniocaudal views of both breasts in a patient with prior silicone injections. Note the multiple high-density nodules of different sizes, with circumscribed borders. Some have calcified contours. Generically, nodules produced by the injection of some substances are called siliconomas. Note also the diffuse subdermal compromise caused by infiltration with silicone gel
On some occasions, they are irregular in shape and have poorly defined edges. As a consequence of fibrosis and the ability to migrate, silicone can be identified in all mammary planes, from subdermal to posterior, even capable of infiltrating the pectoral muscle and axilla [1].
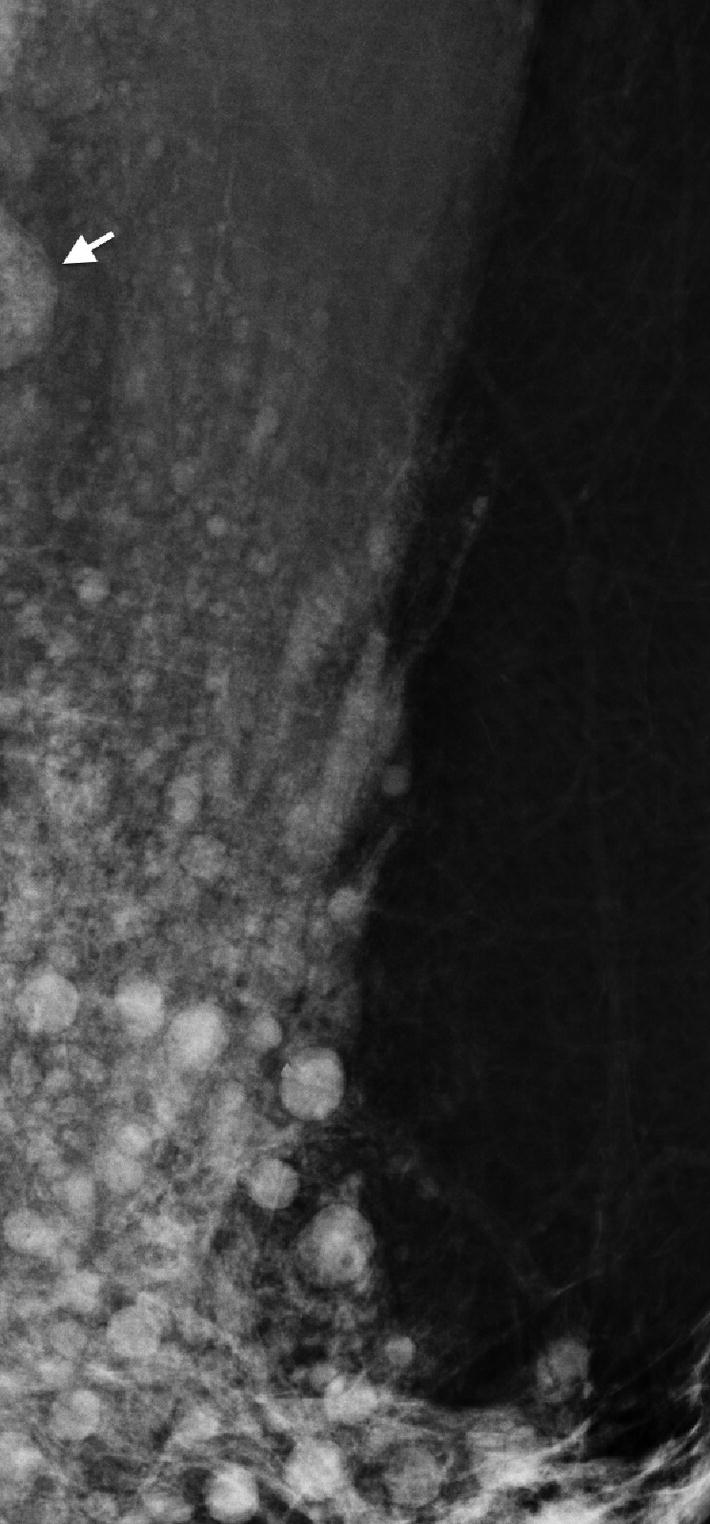
Mammography revealing axillary migration of silicone. Note the numerous siliconomas and infiltration of lymphatic vessels. Note also the partially included high-density lymph node produced by silicone infiltration (arrow)
One limitation of mammography is that it only allows for analysis of the body sector included in the field of study. Given this, it is not possible to evaluate the full extent of siliconomas, since the images exclude, for example, the intermammary groove, thoracic wall, and abdomen.
The other limitation of mammography, which is highly clinically significant, is determined by the high density of siliconomas and their diffuse infiltration throughout the breast. In this way, they can totally obscure other lesions — like nodules, distortions, and microcalcifications — that otherwise would raise suspicions pertaining to other potentially more ominous conditions [2, 4]. This radiological behavior makes it difficult or even impossible for mammography to detect small cancers, which renders it essentially useless for oncological screening in patients with prior silicone injections [11].
Mammary Ultrasound
Patients with a history of silicone injection may be referred for mammary ultrasonography as a screening examination or for clinical symptoms or signs. Among the most common symptoms and signs are one or more palpable abnormalities, painful breasts, and changes in the skin [13]. Like mammography, breast ultrasound is a method that, in these patients, cannot exclude neoplastic mammary pathology [11].
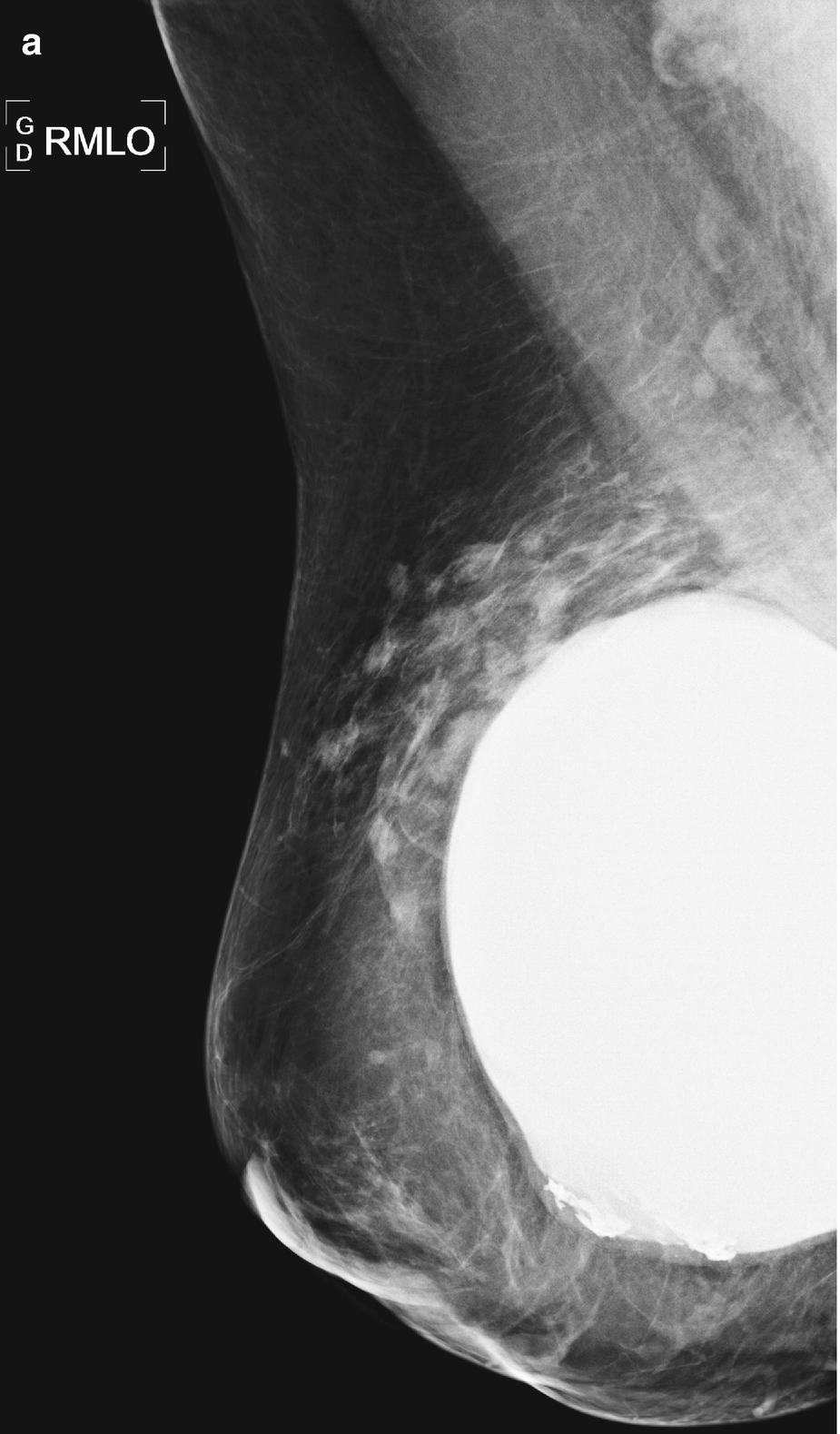
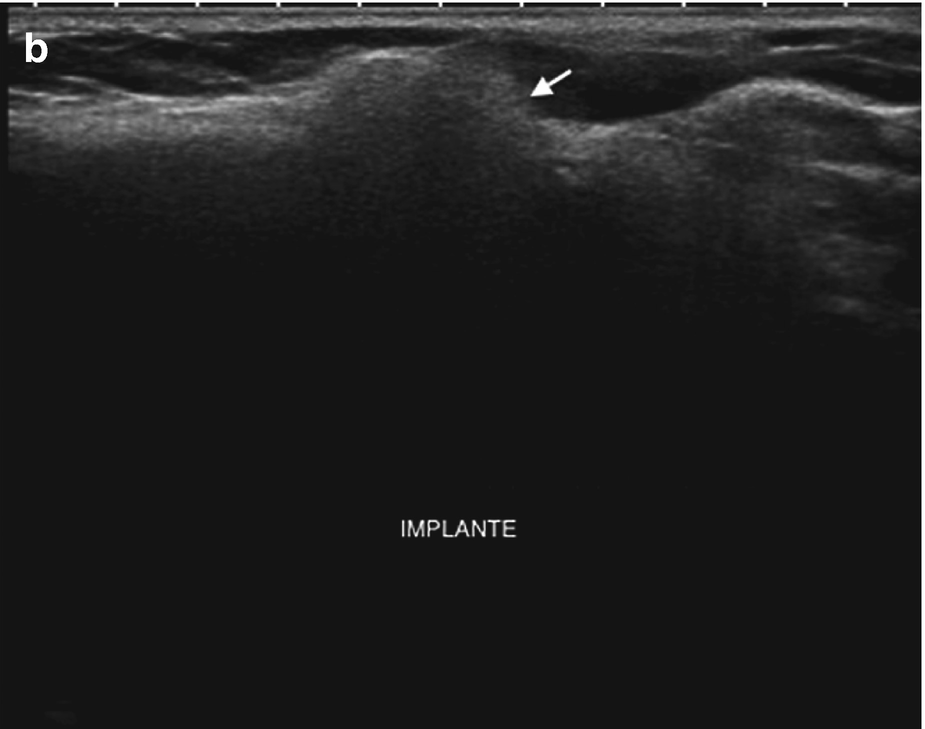
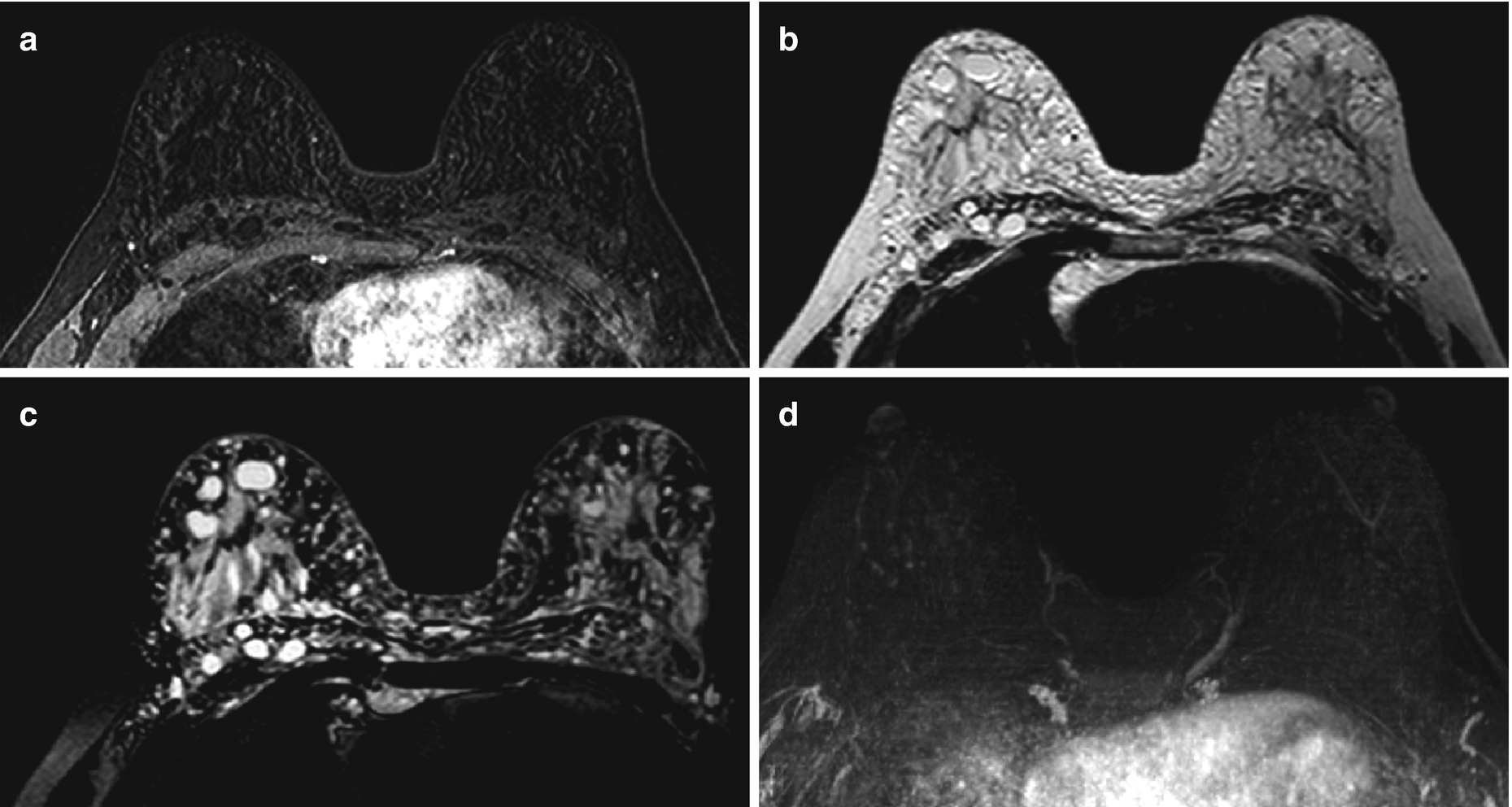
Silicone granuloma (siliconoma) associated with a breast implant. (a) Mammography: siliconomas adjacent to a breast implant. By mammography, it is impossible to determine whether they correspond to an extracapsular rupture or to residual siliconomas secondary to prosthesis replacement. (b) Ultrasound: nodular siliconomas that are echogenic, accompanied by the classic “snowstorm” sign. In this case, ultrasonography demonstrates how the siliconomas are, in fact, residual siliconomas after prosthesis replacement. Note the anechoic structure of the new implant, which determines its integrity
However, not all free silicone in breast parenchyma produces a snowy appearance. In fact, there is a spectrum of ultrasonographic manifestations of silicone granulomas that present in this type of patient [14]. Some silicone collections initially present as complex cysts. The next phase is as a solid iso-echogenic nodule. The third phase is as the classic snowfall, which is a fibrotic reaction to a foreign body (in this case, the silicone). Such nodules can appear spiculated on mammography and cause subsequent acoustic shadowing on ultrasound, similar to lesions suspected of malignancy [15].

Mammary ultrasound corresponding to the mammography images depicted in Fig. 4.1. Note the generalized “snowstorm” sign, produced by a fibrous reaction to the presence of silicone gel, which prevents ultrasonographic recognition of anatomical mammary glandular tissue structures in both the superficial and deep planes. Granulomas coexist in different evolutionary stages; in this case, small siliconomas in their “cystic phase” are identified
The sign of the “snowstorm” occurs in granulomas with smaller silicone globules and a greater foreign body fibrotic reaction. The smaller silicone globules intermingle with the fibrosis and affect the ultrasound beam to a greater extent. The innumerable interfaces between the fibrous tissue, which transmits sound at 1540 m/s, and the silicone drops, which transmit it more slowly, lead to reflection and refraction of the ultrasound beam. The reflections from these innumerable interfaces make the silicone granulomas hyperechogenic; meanwhile, the refractions render the ultrasound beam incoherent, which causes a “dirty” shadow distal to the siliconoma and manifests in the image as a snowfall [15].
The ultrasound scan must necessarily extend beyond the limits of the breast to include the thoracic wall and the axilla, due to the ability of silicone to migrate frequently to these locations. The sonographic findings there will be similar to the previously described “snowstorm.” [16]
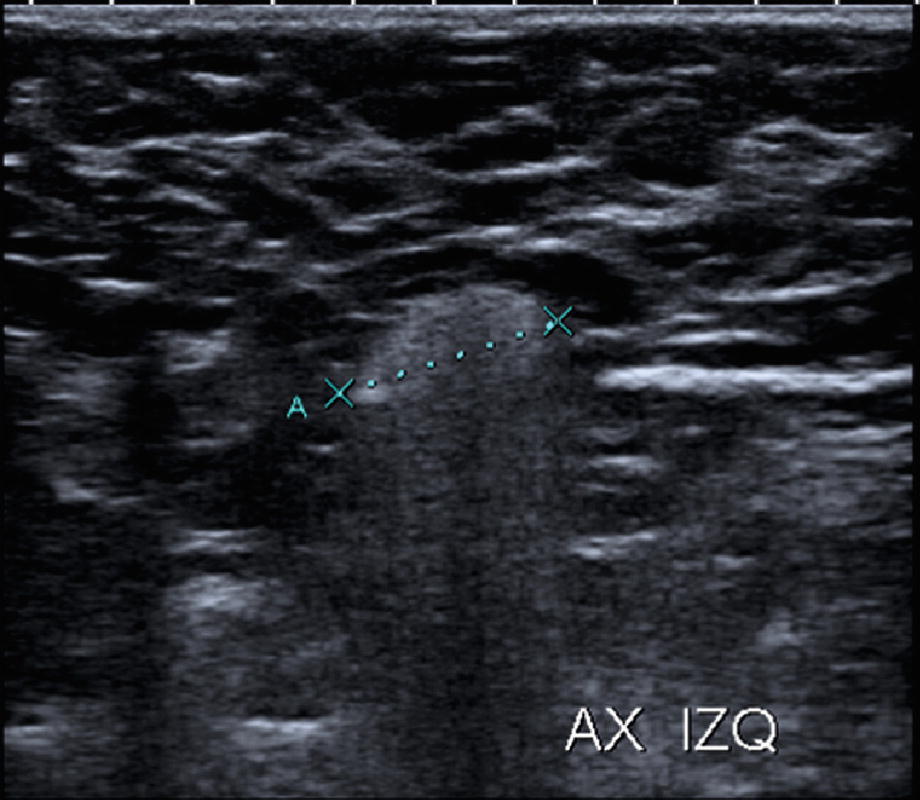
Ultrasound of the axillary region. Note the left axillary echogenic appearance with loss of the normal cortico-hilar relationship and later “snowstorm” sign, produced by the migration of silicone
In patients with a history of liquid silicone injection, granulomas in different stages are scattered throughout the parenchyma, but the “snowstorm” sign predominates, which causes the loss of definition for the evaluation of posterior tissue and renders ultrasonography virtually useless for the detection of suspected neoplasms [2].
Breast Magnetic Resonance Imaging
Compared to mammography and breast ultrasound, contrast-enhanced MRI is an imaging technique that offers not only information of breast morphology but also on the functional characteristics of breast parenchyma, like its perfusion and ability to be enhanced. Contrary to radiographs, MRI also has the advantage of no ionizing radiation. The former characteristics explain the greater sensitivity that MRI has for the detection of breast cancer relative to the diagnostic methods previously described in this chapter.
Important technical requirements that must be considered to obtain a breast MRI suitable for diagnostic purposes are the strength of the magnetic field (1.5 or 3 T), the use of specific coils, and whether or not an intravenous contrast agent, like gadolinium, is administered [17].
The breast coils have a geometric design that provides a high signal-to-noise ratio in an area that spans both breasts, with extension to the chest wall and the axillae. This is very useful in the evaluation of silicone migration to soft tissues in patients with implants or a history of liquid silicone injection. Other considerations in the design of breast coils include patient comfort and open access for MR-guided markers and biopsies. The study is carried out with the patient in a prone position, which minimizes the effects of respiratory movements [18].
The MRI signal is based on different physical principles that reflect the density of water protons in the tissue and their magnetic interactions with other molecules in their local environment. The MR signal is strongly influenced by these magnetic interactions, affected by how fast protons can return to equilibrium (a process characterized by relaxation times T1 and T2) after receiving a radiofrequency stimulus from an external source (the coil). This translates into glandular tissue (due to its high water content), fat and silicone each having their own distinct frequencies. The usefulness of MRI lies in its ability to suppress or emphasize the various signals generated, which allows clinicians to utilize numerous different sequences.
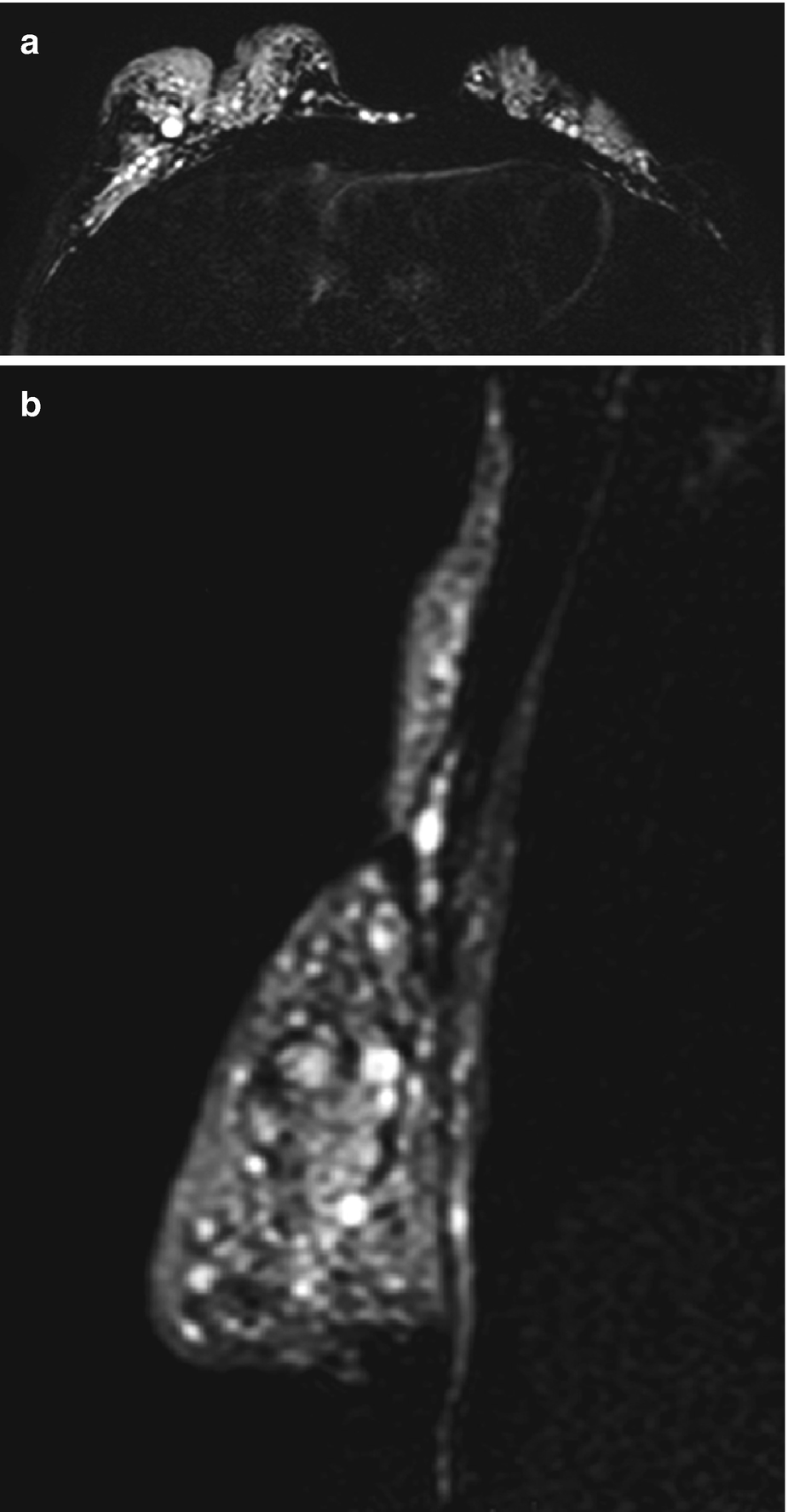
Magnetic resonance imaging (MRI) (a) T2-weighted axial sequence with suppression of fat and water (the so-called silicone-only sequence) reveals deformation and retraction of both breasts, accompanied by the presence of numerous hyperintense siliconomas within the parenchyma, intermammary groove, and chest wall. (b) T2-weighted sagittal sequence with suppression of fat and water (“silicone-only”) clearly demonstrating silicone infiltration of the parenchyma, axillary region, and thoracic wall
Other sequences used to study breasts containing silicone are T2-weighed, axial, and sagittal, where the silicone is isointense with the fat, while water is hyperintense. This sequence is useful for assessing breast implants [2, 17, 18].
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


