Introduction
The iliac crest provides a good source of bone and is universally accepted as a donor site for non-vascularized grafts. Its role as a vascularized graft for head and neck reconstruction has very much decreased in popularity since Hidalgo described the fibula flap for mandibular reconstruction in 1989. There is no doubt that the excellent depth and width of the bone as well as the natural curvature can be an advantage, but the donor site is often quoted as much less favorable to either the fibula or scapula. It has a definite role in the reconstruction of the maxillary defect especially when combined as a myo-osseous flap with internal oblique in Class III defects involving the orbital floor.
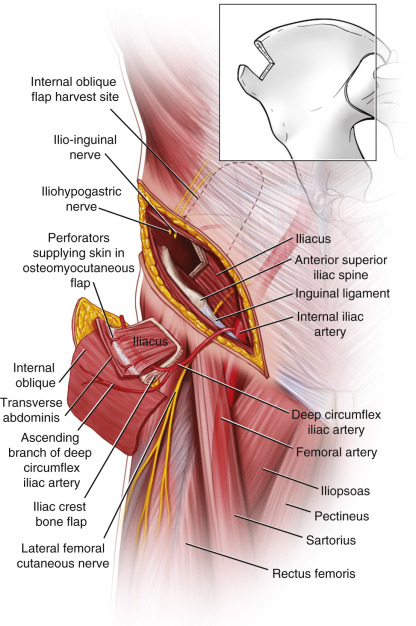
Initially, the flap was raised on the superficial circumflex vessels but now the deep circumflex artery and vein are routinely used. This author prefers always to include the ascending branch to the internal oblique to ensure a dual blood supply through these vessels and the deep circumflex iliac artery (DCIA). The length of the pedicle is reasonable but can be lengthened by not including the anterior superior iliac spine (ASIS) and making the anterior cut more posterior/lateral to the origin of the pedicle.
The skin component can be harvested as a perforator flap based on the deep circumflex iliac artery or as a osteocutaneous flap including iliac bone and the abdominal skin overlying the perforators, which can be placed with more flexibility often combined with internal oblique muscle to add a chimeric option for more complex mandibular and maxillary defects. This is a valid alternative for patients with arterial disease or abnormal lower limb anatomy, which may preclude a fibula option.
Flap Anatomy (see Fig. 42.1 and Fig 11.3 , Fig 11.6 , Fig 11.8 , Fig 11.9 , Fig 11.10 )
Arterial Supply of the Flap (see Fig. 42.1 and Fig 11.6 , Fig 11.9 , Fig 11.10 )
Dominant:
deep circumflex iliac artery (DCIA)
Length: 6 cm (range 5–7 cm)
Diameter: 2.8 mm (range 2–3 mm)
The DCIA is the dominant supply to this flap, which includes the ascending branch, which is the main supply to the internal oblique muscle. The DCIA arises from the external iliac artery superior to the inguinal ligament and passes inferior to the internal oblique muscle in the fascia separating this muscle from the iliacus. The artery gives off the ascending branch at a variable distance from the external iliac to the ASIS (65% within 1 cm and 15% between 2 and 4 cm), and in some cases may not be obvious. This is quoted as high as 20% but in the author’s experience, this is much lower, at between 5% and 10%. Occasionally, I have found that the ascending branch and accompanying vein arise separately from the external iliac system (<5%). There will be communicating branches to the internal oblique from the DCIA, but it is worth soft clamping the ascending system to check that the internal oblique muscle is still supplied. One of my colleagues anastomosed both sets of vessels, but this will depend on the number of recipient options and an alternative soft tissue flap may be required.
The DCIA then lies between the transversalis and iliacus but does not persist in this position starting 2 cm below the iliac crest ridge before passing superiorly over the crest at a variable distance from the ASIS. The DCIA pierces the transversus abdominis muscle approximately 6–9 cm from the ASIS and terminates by anastomosing with the iliolumbar, superior gluteal, and intercostal systems. It is essential when harvesting this flap to maintain the ascending branch to the internal oblique to ensure supply to the bone through this muscle if a long bone harvest of >10 cm is required. Maintaining the internal oblique with its blood supply will ensure a better supply to the distal segment of bone if an osteotomy is required to shape the mandible or maxilla. The deep circumflex iliac vein (DCIV) accompanies the artery initially as venae comitans but these usually merge to leave a single vein draining in to the external iliac vein. The vein tends to pass inferiorly as the dissection approaches the external iliac vein and either passes over or under the artery. If the pathway is over the artery, it is possible to achieve more length to the vein but this is not generally advised if the vein passes inferior to the artery.
The author’s favorite use of this flap is with internal oblique, as described by Urken after the relationship of the internal oblique muscle was explained by Ramasastry et al. It is possible to use a skin island either raised with external oblique, internal oblique, and transversalis but this makes the flap very heavy and bulky for orofacial reconstruction, and the introduction of the skin island as a perforator flap by Kimata et al. has increased the options and versatility of the flap. The site, size and position of the perforators has been mapped by Bergeron et al. and these are generally situated superior to the iliac crest by 4 cm and between 5 and 11 cm posterior to the ASIS. It is possible to check for these with color flow Doppler and handheld Doppler techniques for planning the position of the skin island and to ensure a reasonable size of perforator vessel. Kimata et al. succeeded in raising 7 out of 10 flaps, and so there is a reasonable chance that this chimeric option may not be available. It is not known at this time whether the color flow Doppler or arteriography will accurately predict the usability of this option.
Common Anatomic Variants
- •
The DCIA may arise from the external iliac very close to the inguinal ligament, which will need to be released from the ASIS to ensure access for the dissection.
- •
The ascending branch may be absent, in which case the supply to the internal oblique will be through multiple smaller branches and can still be harvested.
- •
There may be a separate run-off of the ascending branch from the external iliac, which may require an additional set of anastomoses although I have transferred the flap safely without this additional surgery.
Minor:
superficial circumflex iliac artery (SCIA)
Length: 3 cm (range 2–4 cm)
Diameter: 1.5 mm (range 1–2 mm)
The DCIA and SCIA communicate in the region of the iliac crest. The SCIA supplies a small segment of iliac crest bone, usually at the ASIS. The SCIA predominantly supplies the skin anterior and superior to the ASIS and may be used to support a larger skin paddle than may be reliably supplied by the DCIA alone, or may provide vascular supply for an independent and/or additional skin paddle.
Venous Drainage of the Flap (See Figs 11.6 , 11.8 )
Primary:
deep circumflex iliac vein
Length: 9 cm (range 8–10 cm)
Diameter: 3.6 mm (range 2–5 mm)
The deep circumflex iliac venous system parallels the course of the artery before merging with either the femoral vein or the external iliac vein. The two venae comitantes usually diverge superiorly from the artery to coalesce and form the deep circumflex iliac vein (DCIV) approximately 1–4 cm (average 2 cm) from either the femoral or external iliac artery or, more frequently, the external iliac vein beneath the inguinal ligament. The DCIV receives contributions from the superficial system, which will allow drainage of the SCIA territory by the DCIV. The DCIV is usually 2–5 mm in diameter.
Secondary:
superficial circumflex iliac vein
Length: 3 cm (range 2–4 cm)
Diameter: 2.5 mm (range 2–3 mm)
Additional venous drainage of the skin component of the flap may be provided via the paired venae comitantes that accompany the SCIA.
Flap Innervation (See Fig. 42.1 , and Fig 11.9 , Fig 11.10 )
Sensory:
the sensory innervation to skin overlying the iliac crest primarily comes from T12.
The ilio-inguinal nerve (L1) crosses the DCIA and provides sensation to the groin. The genital and femoral branches of the genitofemoral nerve (L1, 2) confer sensibility to the mid-inguinal region and the genital regions, respectively. The lateral femoral cutaneous nerve (L2, 3) courses along the inner surface of the iliacus muscle and penetrates the deep fascia of the thigh about 2 cm inferomedial to the ASIS, providing sensation to the anterior thigh. The DCIA usually crosses over the lateral femoral cutaneous nerve near the ASIS and every effort should be made to preserve the nerve during flap dissection. It may be possible to create a sensate flap based on this nerve, but this technique is not commonly practiced.
Motor:
this flap does not provide for motor reinnervation.
Flap Components
The iliac crest is an excellent source of cancellous bone with a dual blood supply directly to the bone from the DCIA and via the internal oblique through the ascending branch. The best use of the flap is with internal oblique muscle to provide a natural oral lining or grafted muscle. A composite flap without a perforator option is now less commonly used but the perforator option allows versatility in a truly chimeric flap with bone muscle and skin for complex orofacial reconstructions.
Advantages
- •
Excellent bone stock with options for full facial and dental rehabilitation.
- •
Two-team operating.
- •
The ability to close the skin directly without grafting when using a composite flap.
- •
The donor site scar is in a favorable position and can be covered easily.
- •
The natural contour of the bone is favorable for ipsilateral mandibular and maxillary reconstruction.
- •
The internal oblique muscle epithelializes leaving a natural looking result suitable for implant placement.
- •
The perforator flap with internal oblique offers a chimeric flap option for complex cases.
Disadvantages
- •
There is a higher flap failure in some series, which is related to the potential for vessel spasm and the smaller vessels when compared to fibula, scapula, and radial artery.
- •
There is a higher potential for bleeding and the abdominal contents can be damaged if due care is not taken with the flap harvest technique.
- •
Although hernia formation has been cited as a disadvantage of this flap, this is unlikely with careful closure and the use of mesh to support the abdominal wall.
- •
The donor site morbidity can be reduced by raising a split iliac crest only including the abdominal cortex but the iliac deformity is well tolerated and the thickness of the bone important in the primary site.
- •
Sensory loss of the lateral thigh is a potential problem if the lateral femoral cutaneous nerve is injured. However, if this does happen it is generally well tolerated.
- •
Gait disturbance may also occur, particularly when large bony and muscle components are harvested.
Preoperative Preparation
If the patient has a clear medical history and examination of the abdomen is normal, then there are no particular investigations that are required prior to using this flap option. In general, this author would be less inclined to use an iliac crest reconstruction in a patient that is obese but this simply makes the harvest more difficult, and use of bone and internal oblique ensures a flap of normal size as adipose tissue is not included. Any form of perforator and certainly the composite option for such patients, is to be avoided. I have noted that elderly patients have more problems with this donor site but that is true for all the bone harvest donor sites with perhaps scapula being the best tolerated.
It is important to establish that there has been no history of previous surgery to the donor site such as appendicectomy or hernia repair, as there may be damage or fibrosis affecting the pedicle. This donor site should be avoided for patients with a history of deep vein thrombosis, as there are reconstructive options such as scapula, which are less likely to result in this complication. In general, a history of peripheral vascular disease does not preclude this donor site but in such circumstances, appropriate imaging of the vessels and establishing normal undamaged vessels is essential. Some suggest that patients with chronic obstructive pulmonary disease may have a higher risk of incisional hernia formation due to postoperative coughing.
Flap Design
Anatomic Landmarks ( Figs 42.2 , 42.3 )
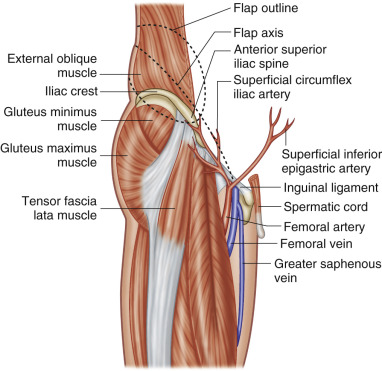
The ASIS, the pubic tubercle, the line of the inguinal ligament, the curve of the iliac crest, the costal margin, and the position of the iliac vessels will help guide the surgeon in planning the incision and skin island if required.
General Thoughts About Flap Design
The position of the internal oblique is planned to decide how posterior the muscle will be harvested, which relates to the position of the bone cuts. The use of a composite flap including a skin island with similar sized harvest of the external oblique, internal oblique, and transversalis muscle is no longer routine practice, as this makes the skin island very bulky with little choice about its placement in relation to the bone. If skin is also required, a perforator skin island is planned and I would use color flow Doppler to establish the presence of a reasonably sized perforator artery in a favorable position and follow this up with a handheld Doppler in the operating room. The perforators have been mapped and are shown to arise from 5–11 cm posterior to the ASIS and about 4 cm above the crest. In a series of 10 cases of perforator iliac crest flaps, Kimata reported only seven successfully harvested.
It is preferred to keep the ASIS with its attachments including the inguinal ligament and not include them in the flap, unless a long span of mandible is being reconstructed and the additional length is required.
Special Considerations
Flap Design Based on Recipient Requirements
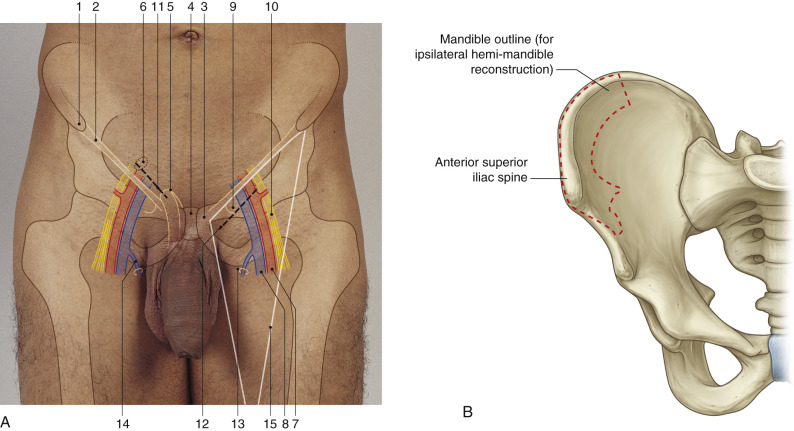
The ipsilateral donor site is preferred for the mandible with the crest forming the lower border and the pedicle emerging posteriorly in relation to the defect ( Fig. 42.2B ). Ipsilateral harvest is also preferred for the maxilla with the crest forming the alveolar part of the reconstruction and the pedicle arising posteriorly. The natural curvature of the iliac crest helps to reduce the need for multiple osteotomies. If a perforator flap is being planned, then the ipsilateral donor site is ideal for external skin requirements using internal oblique intraorally. If there is a very large intraoral defect requiring skin as a reconstruction, then a contralateral donor site may be preferred to allow easier placement of the skin island at a cost of increased osteotomies to accommodate the adverse shape of the ilium. If extraoral skin and intraoral skin are required, then an alternative flap or combined flap option may be the best option.
In tibial reconstruction the direction of the vascular pedicle and limited length of the straight portion of the iliac crest bone suggest that the ipsilateral crest is used if the recipient artery is to be the anterior tibial artery and the contralateral crest is used if the recipient artery is to be the posterior tibial artery.
Difference in Design, if Any, When Performing the Flap as Pedicled or Free
Pedicled bone vascularized iliac flaps have been performed for the treatment of acetabular problems. The design and outline of pedicled flaps from this region would allow for a wide arc of rotation by designing the marks of the flap as far as possible from the origin of the vessels. In addition, a long bone flap is usually required to reach the posterior acetabulum.
Flap Dimensions
Skin Island Dimensions
Length: 15 cm (range up to 20 cm), maximum to close primarily: 20 cm
Width: 8–10 cm (range up to 20 cm), maximum to close primarily: 12 cm
Thickness: variable, depending on the amount of subcutaneous adipose tissue
Muscle Dimensions
Length: 10 cm (range 10–15 cm)
Width: 6 cm (range 6–8 cm)
Thickness: 1 cm (range 0.5–1 cm)
Bone Dimensions
Length: 7 cm (range up to 16 cm)
Height: 4 cm (range 2–7 cm)
Thickness: 1 cm (range 1–1.5 cm, full-thickness bone)
The iliac crest flap can supply a large quantity of bone, up to 16 cm in length. For mandibular reconstruction, a height of about 2.5 cm is appropriate. The thickness of the bone harvested depends on whether the flap is raised as a unicortical, split-thickness bone flap, or a full-thickness bone flap that includes both cortices and the medullary bone. In most cases, the full thickness of the iliac crest is harvested as a thinner flap will reduce the options for implant-retained prosthetic oral rehabilitation. I am not aware of a comparative series observing the donor site outcome with and without the full-thickness harvest, although it is logical to assume that keeping the outer cortex will be an advantage in donor site morbidity. If skin is required, a flap can be 6–12 cm in width and 15–20 cm in length (average 8 × 18 cm) in order to permit primary donor site closure.
Flap Markings ( Fig. 42.3 )
ASIS, iliac crest, internal oblique muscle, costal margin, iliac vessels, inguinal ligament, and proposed skin island make up the usual skin marking. The incision is placed 2 cm above the inguinal ligament and iliac crest, from the iliac vessels to the distal proposed bone cut. The skin island position depends on the result of the color flow Doppler, and handheld Doppler studies but is usually positioned from 5–11 cm posterior to the ASIS and 4 cm above the iliac crest.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


