Homeotherms, including humans, are able to maintain a relatively constant temperature despite variations in their thermal environment. We normally maintain a narrow thermoregulatory threshold range of approximately 0.2°C, and little change in core temperature is required to trigger compensatory mechanisms to either cool or warm our core temperature back to normothermia. This article focuses on the mechanisms and consequences of hypothermia and hyperthermia in the surgical patient and reviews techniques to prevent and treat these conditions.
Key points
- •
Anesthetic medications and techniques can disrupt the thermoregulatory process in surgical patients. Temperature monitoring is essential in patients to preserve normothermia.
- •
Even mild hypothermia may cause bleeding, myocardial events, infection, and postoperative pain.
- •
Untreated, malignant hyperthermia leads to morbidity or death. The perioperative team must be familiar with its diagnosis and prepared with a treatment plan.
- •
Immediate care for malignant hyperthermia demands the ready availability of a cart stocked with dantrolene, diluent, and adjunctive treatment drugs.
- •
A patient with malignant hyperthermia requires continued postoperative care and, if necessary, transfer to an acute care facility.
Homeotherms, including humans, are able to maintain a relatively constant temperature despite variations in their thermal environment. We normally maintain a narrow thermoregulatory threshold range of approximately 0.2°C, and little change in core temperature is required to trigger compensatory mechanisms to either cool or warm our core temperature back to normothermia. This article focuses on the mechanisms and consequences of hypothermia and hyperthermia in the surgical patient and reviews techniques to prevent and treat these conditions.
Normal regulatory mechanisms
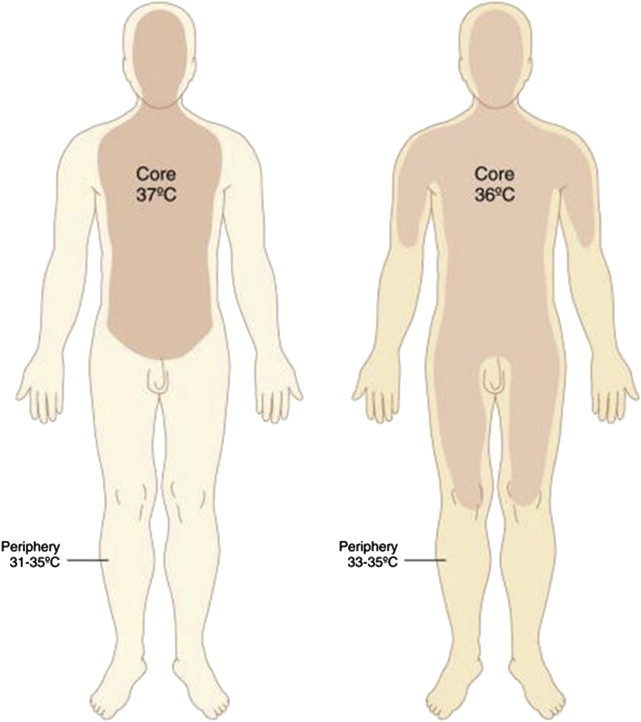
Maintaining core temperature is a complex process. Initially, the hypothalamus was believed to be primarily responsible for temperature regulation, but it has since become clear that spinal cord pathways, abdominal organs, and skin surface temperature contribute to the activation of autonomic thermoregulatory mechanisms, including shivering, vasoconstriction, sweating, and vasodilation. The complexity and multiple locations of thermoregulatory control help explain why a wide range of anesthetic medications and techniques can disrupt normal temperature. Vasoconstriction and shivering take place when the core temperature decreases lower than the lower limit of the thermoregulatory threshold, whereas sweating and vasodilation represent a central response to a core temperature that exceeds the upper limit of the thermoregulatory threshold. Peripheral temperature is usually cooler than the core by 2° to 4°C, with the gradient maintained by peripheral vasoconstriction of arteriovenous shunts. Core heat is conserved and heat dissipation to the environment is prevented to maintain normothermia in an unanesthetized person, but thermoregulation and other processes are often disrupted in an anesthetized patient.
Normal regulatory mechanisms
Maintaining core temperature is a complex process. Initially, the hypothalamus was believed to be primarily responsible for temperature regulation, but it has since become clear that spinal cord pathways, abdominal organs, and skin surface temperature contribute to the activation of autonomic thermoregulatory mechanisms, including shivering, vasoconstriction, sweating, and vasodilation. The complexity and multiple locations of thermoregulatory control help explain why a wide range of anesthetic medications and techniques can disrupt normal temperature. Vasoconstriction and shivering take place when the core temperature decreases lower than the lower limit of the thermoregulatory threshold, whereas sweating and vasodilation represent a central response to a core temperature that exceeds the upper limit of the thermoregulatory threshold. Peripheral temperature is usually cooler than the core by 2° to 4°C, with the gradient maintained by peripheral vasoconstriction of arteriovenous shunts. Core heat is conserved and heat dissipation to the environment is prevented to maintain normothermia in an unanesthetized person, but thermoregulation and other processes are often disrupted in an anesthetized patient.
Hypothermia
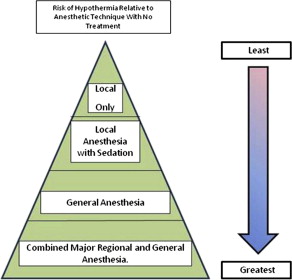
Hypothermia is defined as a core body temperature less than 36°C. Despite an effective homeothermic thermoregulatory system, patients can become hypothermic perioperatively, when the thermoregulatory threshold is widened under the effects of sedation, general anesthesia, or regional anesthesia ( Fig. 1 ).
General Anesthesia
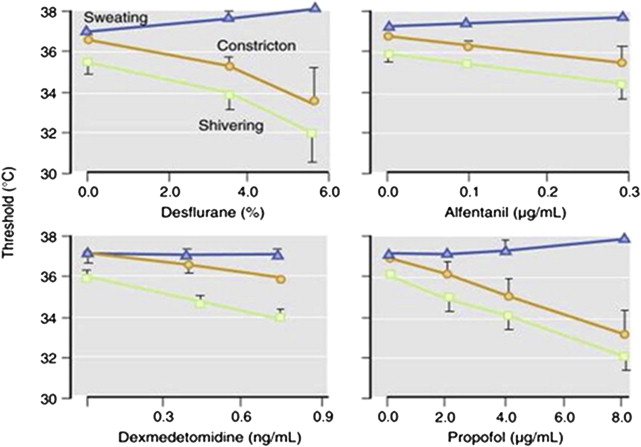
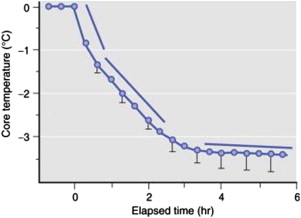
Anesthetic agents disrupt a patient’s normal thermoregulatory mechanisms in different ways, including the loss of behavioral mechanisms (ie, putting on a jacket when cold) because of loss of consciousness to inhibition of autonomic responses, such as shivering and vasoconstriction ( Fig. 2 ). The development of hypothermia during general anesthesia can be described in 3 phases ( Fig. 3 ).
First Phase (Redistribution)
The first or redistribution phase of core temperature heat loss occurs shortly after induction of general anesthesia ( Fig. 4 ). Peripheral vasodilation transfers core body heat to the periphery and subsequently to the environment. With general anesthesia, a core temperature decline fails to trigger normal thermoregulatory vasoconstriction (ie, the body’s thermostat is reset to defend a temperature <37°C). As a result, the normal core/peripheral temperature gradient becomes smaller, with greater heat loss to the environment. Most of the heat loss during a general anesthetic from core/peripheral redistribution occurs within the first hour of the anesthetic and, in the absence of active warming, the patient’s core temperature can decline 1°C to 1.5°C. Redistribution contributes to approximately 80% of heat loss in the first hour, but is not the only contributor. General anesthesia can decrease metabolic heat production by approximately one-third, and exposure to a cool ambient environment, administration of cool intravenous fluids, and the application of cool skin-cleaning solutions can result in up to 5% of additional first-phase heat loss.
Second Phase (Linear)
Without active warming, core temperature declines linearly during the second hour, resulting in the loss of another 1°C to 2°C of core temperature. Core to peripheral heat redistribution contributes only 40% of heat loss during the second phase. Most heat loss during the second phase occurs as a result of decreased metabolic heat production in the setting of cool intravenous fluid administration and the exposure of a large body surface area or large wounds. Heat is lost via radiation, convection, evaporation, and conduction, and outpaces the diminished metabolic heat production during a general anesthetic.
Plateau Phase
The third phase of intraoperative hypothermia is the plateau phase, typically during the third hour of general anesthesia. The plateau phase is characterized by a relatively constant core temperature even with increased surgical time. Heat loss continues, but core temperature is preserved by the restoration of the core/periphery temperature gradient, at a lower temperature, and the activation of autonomic thermoregulatory mechanisms. Plateau phase core temperatures typically reach between 34°C and 35°C.
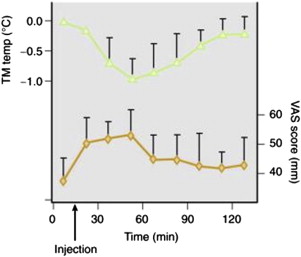
Regional Anesthesia
A major regional anesthetic causes vasodilation and the loss of afferent signaling to the hypothalamus within the affected area. Anesthetized tissue not only loses heat rapidly but also loses heat without signals to the central regulatory system that would activate vasoconstriction and shivering. As a result, patients may subjectively feel warm despite hypothermia ( Fig. 5 ). With vasodilation, redistribution of heat loss is similar to that in the first phase of a general anesthetic and in the case of epidural blockade, core temperature decreases 0.8°C ± 0.3°C during the first hour. Heat loss from redistribution is less than during general anesthesia because part of the body is spared vasodilation, but redistribution remains the primary mechanism of heat loss during regional anesthesia. In the linear phase, heat loss through radiation, convection, evaporation, and conduction may still exceed metabolic heat production, and core temperature may continue to decrease over hours 1 to 3 of the anesthetic. A patient under the influence of a prolonged major regional anesthetic (eg, an epidural block) may not achieve a thermal steady state or plateau phase. Vasoconstriction and shivering do not return during regional anesthesia (as they do during general anesthesia), because of peripheral blockade of the anesthetized area.
Local Anesthesia
Infiltration of a local anesthetic that does not result in major conduction blockade does not affect thermoregulation perioperatively, but many patients who undergo a procedure with infiltration of a local anesthetic also may receive intravenous sedation or analgesia. Opioids and propofol, which disrupt normal thermoregulation, put patients at risk for perioperative hypothermia. Midazolam is unique among anesthetic agents, because it does not seem to appreciably alter thermoregulation. The risk of hypothermia in sedated patients should be considered even if most of the analgesia is provided by infiltration of local anesthetics.
Consequences of Hypothermia
Mild hypothermia can have deleterious effects perioperatively on coagulation, wound healing and infection, patient satisfaction, recovery time, drug metabolism, and the rate of perioperative myocardial events. Although controversy persists regarding the clinical significance of coagulopathy that results from mild hypothermia, the investigators of 1 meta-analysis concluded that mild hypothermia, even a decrease of less than 1°C from core normothermia, is sufficient to increase procedural blood loss by 16%. Mild hypothermia is believed to increase the risk of wound infection by several mechanisms. Vasoconstriction reduces blood flow to wounds, lessening subcutaneous oxygen tension locally and predisposing to wound infection and delayed healing. Hypothermia also may impair immune defenses so that bacterial contamination results in infection. A 2°C core temperature decline from normothermia tripled the rate of wound infection after colon resection, so maintaining normothermia perioperatively has the potential to decrease the chances of a surgical wound infection.
Hypothermia also may affect myocardial events. Although metabolic demand from shivering may have a small effect on myocardial events, increased release of catecholamines in the hypothermic patient may predispose to myocardial events. Patients with hypothermia of less than 2°C had a greater than double risk of a myocardial event than did a normothermic group.
Mild hypothermia also slows the metabolism of many drugs typically used as anesthetic agents. Hypothermia alters the pharmacokinetics of medications such as propofol, neuromuscular blocking agents, and even the volatile anesthetic agents. A decrease in core temperature of 3°C increased propofol plasma concentrations and prolonged duration of neuromuscular blockade with atracurium. A hypothermic patient may suffer from delayed awakening and a longer duration of neuromuscular blockade. Mildly hypothermic patients may increase metabolic heat production by shivering postoperatively, an unpleasant sensation for most people and even more so when postoperative wounds are fresh. As a result, postoperative hypothermia may contribute to patient dissatisfaction and prolong the recovery period.
The consequences of mild perioperative hypothermia have led to policies to encourage the maintenance of perioperative normothermia. The basic monitoring standards of the American Society of Anesthesiologists state that “every patient receiving anesthesia shall have temperature monitored when clinically significant changes in body temperature are intended, anticipated or suspected.” An American Society of Plastic Surgeons task force on patient safety advised that office-based facilities have temperature monitoring equipment and the ability to adjust temperature and actively warm patients. Facilities that do not have such capabilities should accept patients only for procedures expected to last 2 hours or less that involve no more than 20% of the body surface area. The standards of the Surgical Care Improvement Project require that patients have at least 1 documented temperature of 36°C within the 30 minutes before or 15 minutes after the documented anesthesia end time or the documented use of active warming intraoperatively. The Center for Medicare and Medicaid Services has also adopted this criterion for reimbursement. Thus, the prevention of perioperative hypothermia not only optimizes patient outcomes, but is used as a metric for institutional performance.
Measurement Devices and Techniques
Maintaining normothermia and treating hypothermia require reliable and accurate core temperature monitoring, which is not always easy to obtain. An invasive pulmonary artery catheter provides accurate monitoring of core temperature but is impractical for most patients, especially in the ambulatory setting. The direct application of a temperature probe to the tympanic membrane provides a good monitor of core temperature, but more readily available infrared tympanic temperature monitors fail to reliably approximate core temperature unless properly placed directly in front of the tympanic membrane. Nasopharyngeal measurement also reasonably approximates core temperature. Distal measurement of esophageal temperature is a good method of temperature monitoring used by anesthesiologists during a general anesthetic, but for a nonintubated patient, esophageal temperature probes are impractical. Additional measurement sites include the rectum and bladder, but temperature values can be affected by local factors, including urine output. In an ambulatory setting, rectal measurement of temperature can be a good option for patients who undergo a lower body regional anesthetic with attendant perineal blockade.
Cutaneous temperature monitoring may be used as a proxy for core temperature measurement but is better suited for trending than for accuracy. Axillary temperature monitoring works best when the temperature probe is placed over the patient’s axillary artery and the corresponding arm is tucked beside the torso. Adhesive liquid crystal thermometer strips can be useful for core temperature monitoring if placed properly. The skin of the forehead is typically 2°C cooler than the core, and this relationship is well maintained as core temperature changes. Even if an accurate core temperature reading is elusive, monitoring can at least identify a trend of cooling or heating that threatens normothermia.
Preventing Hypothermia
The 2 methods of maintaining a patient’s temperature perioperatively are passive and active warming. Passive techniques prevent the loss of heat without specifically adding any heat to the system. Blankets, surgical drapes, and passively humidified respiratory gases are examples of passive warming. Although passive warming can limit heat loss, it has not been shown to prevent hypothermia.
Unlike passive techniques, active warming adds external heat. Radiant heat lamps, higher ambient (room) temperatures, forced air blankets, and fluid warmers are examples of active warming methods. Forced air warmers are the most commonly used active warming devices. Comparisons of forced air warming devices with passive devices such as cotton blankets and reflective blankets have shown that forced air blankets are superior for maintaining normothermia. To be effective, a forced air blanket must let warmed air circulate and must be in contact with the patient’s body. Peripheral heat content gain during the preoperative phase has been shown to diminish heat loss during the redistribution of heat from the core to the periphery in phase 1 of the intraoperative phase.
Administration of intravenous fluids at room temperature can lower body temperature by 0.25°C per liter, but warmed intravenous fluids can help prevent perioperative hypothermia. The combination of forced air warming and warmed intravenous fluid administration (average 6 L) has been suggested to be superior to forced air warming alone, preventing perioperative hypothermia in major surgery.
Fluids used for irrigation and tumescent infiltration can also contribute to the development of perioperative hypothermia. A comparison of lipoplasty patients treated with cool (27°C) versus heated (37°C) tumescent solution without additional active warming showed both groups to be hypothermic at the end of the 3.5-hour procedure. The group who received heated tumescent solution did maintain a higher mean core temperature (35.7°C) than the group who received cool tumescence (34.9°C), showing that warming infiltration fluids does not prevent hypothermia without other active measures. Also, procedures that require large amounts of irrigation fluid or tumescent solution often result in exposure of greater patient body surface area, which may accelerate patient heat loss perioperatively. Thus, warming solutions for irrigation or infiltration are best used in combination with other active warming techniques, such as forced air warming devices and warm intravenous fluids.
Summary
Most patients undergoing procedures with anesthesia, except those who receive infiltration with local anesthetics only, are at risk of hypothermia. Even mild hypothermia may negatively affect patient outcome by increasing bleeding, myocardial events, wound infections, postoperative pain, and recovery time. The risks of perioperative hypothermia must be recognized, and we must be vigilant in detecting, treating, and preventing it ( Box 1 ). Temperature monitoring is essential to the preservation of patient normothermia. Monitoring is critical in procedures involving major regional anesthetics, because physicians may be unable to detect and patients unable to react to hypothermia. Maintenance of normothermia is best accomplished with the use of forced air warming devices over a sufficient period to minimize loss of core heat. A coordinated effort during the preoperative, intraoperative, and postoperative care phases is essential for preventing hypothermia.
Related posts:
 Conscious Sedation/Local Anesthesia in the Office-Based Surgical and Procedural Facility
Conscious Sedation/Local Anesthesia in the Office-Based Surgical and Procedural Facility
 Deep Vein Thrombosis Chemoprophylaxis in Plastic Surgery
Deep Vein Thrombosis Chemoprophylaxis in Plastic Surgery
 Airway Management in the Outpatient Setting
Airway Management in the Outpatient Setting
 Outpatient Surgery and Sequelae
Outpatient Surgery and Sequelae
 Management of Postoperative Nausea and Vomiting in Ambulatory Surgery
Preventing Surgical Mishaps
Management of Postoperative Nausea and Vomiting in Ambulatory Surgery
Preventing Surgical Mishaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


