66
Human Papillomaviruses
Key Points
• Different genotypes cause different skin lesions (Table 66.1).
Table 66.1
Clinical manifestations of common human papillomavirus (HPV) types.
In clinical practice, subtyping is generally only performed routinely on Papanicolaou smears. Subtyping does not usually change management of cutaneous lesions.
| Skin Lesions | Frequently Detected HPV Type |
| Common, palmar, plantar, myrmecial warts | 1, 2, 4 |
| Flat warts | 3, 10 |
| Epidermodysplasia verruciformis | 5, 8* > others (e.g. 9, 20) |
| Condylomata acuminata (anogenital warts) | 6, 11 |
| High-grade squamous intraepithelial neoplasia (cervical lesions, bowenoid papulosis, erythroplasia of Queyrat) | 16, 18, 31, 33 > others (e.g. 35) |
| Cervical cancer | 16, 18 |
* Oncogenic, like HPV types 16, 18.
– Transmitted via person-to-person contact or contact with contaminated surfaces/objects.
– Numerous warts or persistent/progressive warts should prompt consideration of immunosuppression, defects in cellular immunity, or other syndromes [e.g. HIV infection, epidermodysplasia verruciformis, WHIM syndrome (see Chapter 49)].
• Anogenital infection with HPV.
• Rx.
– If desired, focuses on destruction of visible lesions or induction of an immune response.
– Effective targeted antiviral treatments are not available.
Common Warts (Verrucae Vulgares)
• Any site, but commonly on the fingers, dorsal hands, and/or sites prone to trauma (Figs. 66.1 and 66.2).



Fig. 66.2 Periungual common warts. Destruction of the nail matrix and bed can lead to partial (A) or complete (B) absence of the nail plate. Bowen’s disease may be considered in the differential diagnosis, especially for a single, recalcitrant digital wart. A, B, Courtesy, Reinhard Kirnbauer, MD, and Petra Lenz, MD.
• Hyperkeratotic, exophytic or dome-shaped papules or plaques with punctate black dots (thrombosed capillaries) that may require paring to see (Fig. 66.3).

• Rx: outlined in Fig. 66.4; may regress spontaneously within 1–2 years; may be difficult to eradicate.
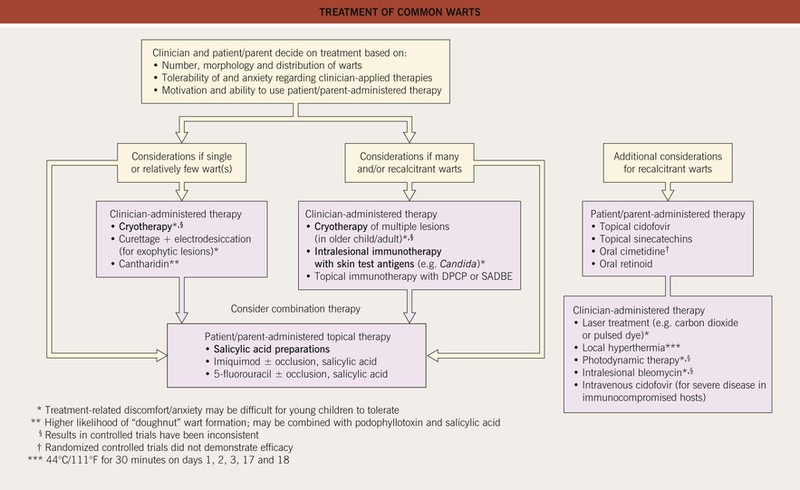
Fig. 66.4
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


