A parent has lymphedema
Turner syndrome, Noonan syndrome
Cancer treatment with inguinal/axillary lymphadenectomy or radiation
Travel to areas endemic for filariasis
Extreme obesity
Onset several months after injury to the lymphatic system
Progressive enlargement of the area
Cellulitis
Minimal discomfort
Symptoms
The most common problem caused by lymphedema is lowered self-esteem because the disease creates a deformity. Consequently, patients often cover their extremities and avoid activities that would expose their abnormal limb to others (e.g., swimming, wearing shorts). The condition also continually reminds cancer survivors of their malignancy. Genital lymphedema can negatively affect a patient’s sexual activity. The second most common morbidity of lymphedema is infection. Patients often state that they have had cellulitis of the involved area, and many have required inpatient intravenous antibiotics.
Lymphedema typically is painless; if a patient complains of significant pain it is unlikely he/she has the condition. As the size of the extremity enlarges, however, secondary musculoskeletal discomfort can occur. Patients often state that the extremity feels heavy, and some individuals have decreased cutaneous sensation. Lymphedema only affects the skin and subcutaneous tissue leading to circumferential overgrowth. The disease does not involve the muscles or bone, and thus, patients do not have axial overgrowth and a leg-length discrepancy. Individuals with severe overgrowth can have difficulty fitting clothing and using the enlarged limb. It can be hard to lift a lymphedematous upper extremity when getting dressed. A markedly enlarged lower extremity can inhibit ambulation. Lymphatic vesicles may bleed or leak lymph fluid (lymphorrhea). Cutaneous ulceration is not typical for lymphedema and should suggest an alternate diagnosis (e.g., venous insufficiency).
Physical Examination
Location
The anatomical distribution of lymphedema includes: an extremity (99 %), isolated genitalia (1 %), or localized to another area of the body (<1 %). Lymphedema almost always affects the distal extremity; if the hand or foot is not involved, then the diagnosis of lymphedema should be questioned. If a patient complains of swelling outside of the limbs or genitalia, then lymphedema likely is not the cause. However, primary generalized lymphedema (including the face and trunk) can occur rarely. Children or adults with secondary lymphedema have lymphedema of the extremity ipsilateral to the site of axillary/inguinal lymph node injury.
Primary lymphedema affects the lower extremities in 92 % of cases; 50 % have unilateral lymphedema and 50 % have bilateral disease [3]. Eighteen percent of patients with primary lymphedema have genital involvement, which usually is associated with lower extremity lymphedema (4 % have isolated genital disease). Sixteen percent of children with idiopathic lymphedema have upper extremity disease [3]. Rarely, a child can have lymphedema affecting the legs, genitalia, and/or arms. Approximately 2/3 of patents with lymphedema in infancy have bilateral lower extremity disease, while 2/3 of patients who present in adolescence have unilateral lower extremity lymphedema [3].
Severity
Clinically, the severity of lymphedema can be categorized as mild (<20 % increase in extremity volume), moderate (20–40 %), or severe (>40 %) (Fig. 10.1) [19]. Limb volume measurements can be made using a tape measure, perometer or by water displacement. Tape measurements are the least accurate method to determine extremity volume because it must be calculated; it is also difficult to use the exact reference points for future assessments. In addition, depending on how tight the examiner pulls the tape measure the circumference can change significantly. In children, extremity measurements are particularly problematic because the limbs are still growing. We do not routinely record limb volumes because it does not affect the patient’s management. However, an individual who is being considered for operative intervention undergoes water displacement to assess extremity volume before and after the procedure.

Fig. 10.1
Severity of lymphedema. (Left) mild. (Center) moderate. (Right) severe
Pitting Edema
Patients with lymphedema exhibit pitting edema early in their disease. Even minor swelling can be appreciated because superficial veins are less visible (Fig. 10.2). Pressing the thumb into the dorsum of the hand or foot for 60 s will illustrate the degree of pitting edema (Fig. 10.3) [20]. Significant pitting (measured in millimeters) indicates that fluid is primarily responsible for limb enlargement and the patient can be managed using compression (Grade 1 edema) [20]. Over time, the body reacts to the lymphedematous fluid in the extremity by producing subcutaneous fibro-adipose tissue. Consequently, on physical examination the amount of pitting edema is reduced. Individuals with long-standing lymphedema may not exhibit pitting edema on physical examination (Grade 2 edema); these patients will have minimal benefit from conservative interventions and are candidates for surgical excisional procedures [20].


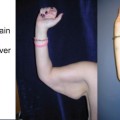
Fig. 10.2
Lymphedema of the right arm causes superficial veins to be less visible
Fig. 10.3
Pitting edema in early lymphedema
Stemmer Sign
A fairly sensitive and specific sign for lymphedema is the Stemmer sign [21]. If the examiner is unable to pinch the skin on the dorsum of the hand or foot (positive Stemmer sign), then it is likely the patient has lymphedema (Figs. 10.4 and 10.5




Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
